[Antibiogramm von Bakterien, isoliert von der Tastatur von Geldautomaten in Hamadan, West-Iran]
Hassan Mahmoudi 1Mohammad Reza Arabestani 1
Mohammad Yousef Alikhani 1,2
Iraj Sedighi 3
Hamed Farhadi Kohan 1
Mohammad Molavi 1
1 Microbiology Department, Hamadan University of Medical Sciences, Hamadan, Iran
2 Brucellosis Research Center, Hamadan University of Medical Sciences, Hamadan, Iran
3 Pediatric Departments, Hamadan University of Medical Sciences, Hamadan, Iran
Zusammenfassung
Zielsetzung: Bakterien sind ubiquitär in der Umwelt verbreitet. Verbunden mit der wachsenden Bevölkerung, der Urbanisation und dem Zeitmangel wächst die Inanspruchnahme von Geldautomaten (ATM). Daher sollten die bakterielle Kontamination und deren Antibiotikaresistenz auf Tastaturen von ATM in der Provinz Hamadan, Iran, untersucht werden.
Methode: Von 360 ATM wurden 96 randomisiert ausgewählt. Die Antibiotikaempfindlichkeit wurde im Agardiffusionstest unter Verwendung von Plättchen mit Gentamicin (10 µg), Vancomycin (30 µg), Trimethoprim/Sulfamethoxazol (25 µg), Amikacin (30 µg), Tobramycin (10 µg), Cephalotin (30 µg), Norfloxacin (5 µg) und Ceftizoxim (30 µg) ermittelt.
Ergebnisse: Die höchste Kontamination wurde bei 18 (27,7%) bzw. 12 (18,5%) der ATMs von Melli und Saderat Banken nachgewiesen. Am häufigsten wurden Staphylococcus epidermidis und Pseudomonas aeruginosa je 12-mal (18,5%), Bacillus subtilis 11-mal (16,9%), Klebsiella spp. 8-mal (12.3%), Escherichia coli und Bacillus cereus je 6-mal (9,2%), Micrococcaceae spp. 5-mal (7,69%), Staphylococcus aureus 3-mal (4,6%) und Enterobacter spp. 2-mal (3,1%) nachgewiesen. Alle isolierten Bakterien waren empfindlich gegen Gentamicin, Cephalotin, Tobramycin, Amikacin, Norfloxacin und Vancomycin. Der Anteil von S. aureus mit Resistenz gegen Trimethoprim/Sulfamethoxazol betrug 50%.
Schlussfolgerung: Alle untersuchten ATM Tastaturen waren mit mindestens einer Bakterienspecies kontaminiert. Daher erscheint es sinnvoll, z.B. nach dem Betreten der Wohnung, des Arbeitsbereichs oder eines Krankenhauses eine Händedesinfektion durchzuführen, um keine kritischen Pathogene in das persönliche Umfeld bzw. in das Krankenhaus einzubringen.
Schlüsselwörter
Geldautomat, Tastatur, bakterielle Kontamination, Antibiogramm
Introduction
Bacteria exist everywhere in the environment and are able to persist or even grow on any surface [1], [2]. Although most bacteria are harmless, some of them are pathogenic, especially in people with weakened immune system. Due to the ongoing development and expansion of urbanization, as well as the increasing population, people do not have enough time to use traditional banking systems and have embraced new developments in electronic banking, such as ATMs (automated teller machines). Today, the extended use of electronic technologies is considered a source of bacterial contamination [3]. In general, microbes can persist or grow on many surfaces, such as those found in restaurant kitchens and hospital environments, as well as on standard office equipment such as computer keyboards, telephones, cellphones, and ATMs [3], [4], [5], [6], [7]. It was estimated that worldwide about 4.2 million ATMs have been used in 1960 [8], [9], [10]. The routine use of these devices involves inserting the card in the machine and using the fingers to enter the password [9]. Phones and devices with metal keyboards are easily contaminated with pathogenic microorganisms, and bacterial colonization and biofilm formation has been investigated by several researchers on metallic surfaces [10], [11], [12]. Today, the presence of electronic devices has increased exponentially in almost all areas of life the environment (playground equipments, ATM keyboards, kitchen sinks, office desks, computer keyboards, escalator handrails, elevator buttons and with the spread of supermarkets and hypermarkets the shopping carts handles). The US Centers for Disease Control and Prevention has estimated that there were 4.5 infections per 100 hospitalizations in 2002 [13], [14], [15]. The aim of this study was to assess the bacterial contamination of ATMs in Hamadan, western Iran.
Materials and methods
Out of 360 ATMs at four locations in Hamadan (number provided by the central bank of the islamic republic of Iran) 96 ATMs were randomly selected. Using a sterile swab soaked in saline, samples were taken from the surfaces of the ATM keyboards. The swab was put into nutrient broth media and transferred to the microbiology laboratory of the University of Medical Sciences, Hamadan and incubated for 30 min. In order to differentiate microorganisms, swabs were cultured on blood agar and MacConkey agar plates and incubated at 37°C for 18–24 hours. Identification of the isolated bacteria was performed using standard microbiological methods [16]. For all isolated strains, antibacterial susceptibility was tested using the standard Kirby-Bauer disk agar diffusion (DAD) method on Mueller Hinton agar (Merk Co., Germany) according to the clinical and laboratory standards institute guidelines (CLSI; 2015, M100-S25) [17] using gentamicin (10 µg), vancomycin (30 µg), trimethoprim/sulfamethoxazole (25 µg), amikacin (30 µg), tobramycin (10 µg), cephalotin (30 µg), norfloxacin (5 µg), and ceftizoxim (30 µg) disks (Mast Co.UK).
All statistical analyses were performed using the SPSS software package, version 21.
Results
A total of 65 positive samples (67.7%) of the ATM keyboards were obtained (Table 1 [Tab. 1]).
Table 1: The frequency of bacterial contamination of ATMs
The most frequently contaminated ATMs belonged to the Melli and Saderat banks, with 18 (27.69%) and 12 (18.46%) cases, respectively (Table 2 [Tab. 2]). The prevalence of isolated bacteria included Escherichia coli on 6 (9.23%) ATM keyboards, Klebsiella spp. on 8 (12.30%), Enterobacter spp. on 2 (3.07%), Bacillus cereus on 6 (9.23%), Bacillus subtilis on 11 (16.92%), Staphylococcus epidermidis on 12 (18.48%), Staphylococcus aureus on 3 (4.61%), Micrococcaceae spp. on 5 (7.69%) and Pseudomonas aeruginosa on 12 (18.64%) keyboards (Table 3 [Tab. 3]). The sensitivity patterns to tested antibiotics are shown in Table 4 [Tab. 4].
Table 2: The number of contaminated ATMs according to banks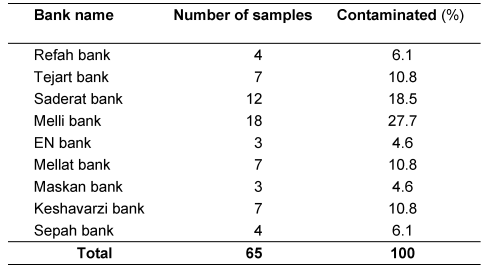
Table 3: Distribution of bacterial species isolated from ATMs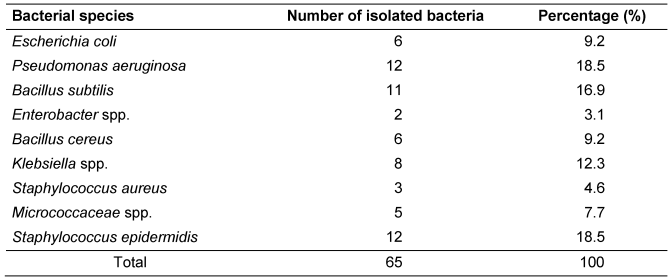
Table 4: Antimicrobial susceptibility patterns of bacterial strains isolated from ATMs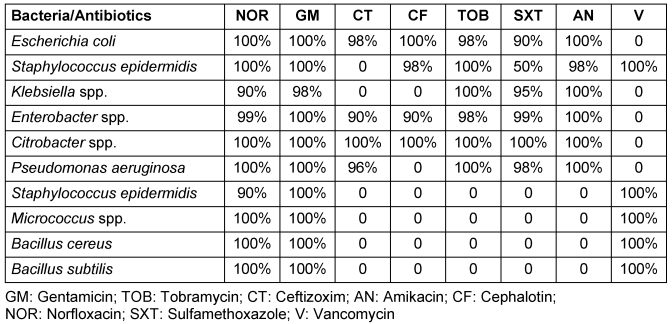
Discussion
The findings of this study showed that ATM keyboards can be considered a source of bacterial infections, similar to other contaminated surfaces in public places, such as telephones and door handles. Because most people with different levels of hygiene and health standards use these machines, they can be widely involved in absorbing, harboring, and transferring infectious microorganisms. Contaminated hands touching an ATM keyboard can transfer pathogens to the keyboard and bills, ultimately facilitating the spread of infectious diseases [12], [13], [14], [15]. In our study, the most commonly isolated microbes were members of the Enterobacteriaceae, especially E. coli as an intestinal pathogen. The results of a study conducted by Gontijo Filho et al. [1] showed that ordinary washing hands cannot eliminate the microorganisms completely; it can only reduce contamination with microbial pathogens. In another study, isolation of Coliforms from coins, paper money, and public telephones has been reported [2]. In research performed by Karabay et al. in Turkey, 111 samples from mobile phones had contamination with microbes that can cause hospital infections. A study in which samples were collected from clothing (e.g. coats, ties) and medical equipment such as stethoscopes and clothing labels, showed microbial contamination [18], [19], [20]. A study by Neely et al. [21] in Ohio, USA on plastic and fabric demonstrated contamination with Enterococcus spp. and Staphylococcus spp. In a study by Ramesh in India [22], of 101 samples collected from mobile phones, 45% were colonized with Gram-positive and 15% with Gram-negative bacteria. Ashgar and El-Said [23] found that 64% of 96 collected swab samples from ATM slots, buttons, and door handles in Mecca city were negative and 26% were positive, a lower percentage than in our study. However, the bacterial spectrum was similar (E. faecalis, Bacillus spp. and E. coli). In a study on external surface of computer keyboards and computer mice, Malik et al. [24] found all samples to be contaminated with pathogenic bacteria (E. coli, Salmonella, Shigella, and Staphylococcus spp.), with E. coli dominating the isolates. Another paper, similar to the current study, showed that ATM surfaces were contaminated by pathogenic bacteria [25]. Furthermore, other authors obtained Gram-positive bacteria from currency notes and computer keyboards [26], and Gram-negative bacteria from hospital curtains, cell phones, hospital staff coats, and ties [26], [27]. Similar to the present study, ATMs in Ebonyi state, Nigeria, were positive for S. aureus, coagulase-negative Staphylococcus, Streptococcus spp., Pseudomonas spp., Enterobacter spp. and E.coli [28]. In our study, the rate of Gram-positive bacteria was higher than that of Gram-negative bacteria. Fazeli et al. [29] isolated P. aeruginosa from the hospital staff, equipment and clinical samples. The isolates from the environmental samples and staff’s hands did not show significant differences in antibiotic resistance patterns [29], but the current study on P. aeruginosa strains isolated from the ATM keyboards showed that they were sensitive to all studied antibiotics. This discrepancy might be due to different geographical locations. The results of the present study are in accordance with those of Abban et al. [9] and Okoro Nworie et al. [30], who reported the presence of Staphylococcus spp., E. coli, and Klebsiella spp. on the keyboards of ATMs. All studies on ATMs demonstrate that they are a possible factor in transmitting infectious diseases.
Conclusions
The results of this study show that some pathogens found on ATM keyboards, such as S. aureus and P. aeruginosa, express resistance to a variety of antibiotics. The ATMs are located throughout town and, especially when near hospitals, are capable of adsorbing and transmitting pathogens. It is imperative that these devices be considered as potential vehicles in the transmission of infections. Since the use of these devices is unrestricted, a health guideline is necessary to prevent infections [5]. There is no practical means of continually disinfecting such equipment. It is questionable that frequent cleaning by an operator would be enough to interrupt cross contamination, because after the next touch, contamination could be as high as before. It appears more feasible to disinfect the hands after entering one’s own apartment, work area, or a hospital, in order to stop the spread of environmentally acquired pathogens to the personal environment or the hospital. This makes sense because a prospective, controlled, intervention-control study implementing untargeted hand disinfection at work places in a public administration significantly reduced common cold, fever, coughing, and diarrhea [31].
Notes
Competing interests
The authors declare that they have no competing interests.
Acknowledgements
This research was financially supported by a grant from Students Research Center, Hamadan University of Medical Sciences.
References
[1] Gontijo Filho PP, Stumpf M, Cardoso CL. Survival of gram-negative and gram-positive bacteria artificially applied on the hands. J Clin Microbiol. 1985 Apr;21(4):652-3.[2] Kramer A, Schwebke I, Kampf G. How long do nosocomial pathogens persist on inanimate surfaces? A systematic review. BMC Infect Dis. 2006 Aug;6:130. DOI: 10.1186/1471-2334-6-130
[3] Saroja V, Kamatchiammal S, Brinda K, Anbazhagi S. Enumeration and Characterisation of Coliforms from Automated Teller Machine (ATM) Centers in Urban Areas. J Modern Biotechnol. 2013;2(1):14-22.
[4] McFarland LV, Mulligan ME, Kwok RY, Stamm WE. Nosocomial acquisition of Clostridium difficile infection. N Engl J Med. 1989 Jan;320(4):204-10. DOI: 10.1056/NEJM198901263200402
[5] Noskin GA, Stosor V, Cooper I, Peterson LR. Recovery of vancomycin-resistant enterococci on fingertips and environmental surfaces. Infect Control Hosp Epidemiol. 1995 Oct;16(10):577-81. DOI: 10.2307/30141097
[6] de Gialluly C, Morange V, de Gialluly E, Loulergue J, van der Mee N, Quentin R. Blood pressure cuff as a potential vector of pathogenic microorganisms: a prospective study in a teaching hospital. Infect Control Hosp Epidemiol. 2006 Sep;27(9):940-3. DOI: 10.1086/507284
[7] Huang R, Mehta S, Weed D, Price CS. Methicillin-resistant Staphylococcus aureus survival on hospital fomites. Infect Control Hosp Epidemiol. 2006 Nov;27(11):1267-9. DOI: 10.1086/507965
[8] Hone K, Graham R, Maguire M, Baber C, Johnson G. Speech technology for automatic teller machines: an investigation of user attitude and performance. Ergonomics. 1998;41:962-81. DOI: 10.1080/001401398186531
[9] Abban S, Tano-Debrah K. Automatic teller machines (ATMs) as potential sources of food-borne pathogens - a case from Ghana. Nat Sci. 2011;9:63-7.
[10] Sosan A, Kinal D. Food pathogens for potential automatic tius machines. Bull Appl Res Sci. 2011;1(2):14-8.
[11] Sharma M, Anand S. Biofilms evaluation as an essential component of HACCP for food/dairy processing industrya case. Food Contr. 2002;13:469-77. DOI: 10.1016/S0956-7135(01)00068-8
[12] Hood SK, Zottola EA. Adherence to stainless steel by foodborne microorganisms during growth in model food systems. Int J Food Microbiol. 1997 Jul 22;37(2-3):145-53. DOI: 10.1016/S0168-1605(97)00071-8
[13] Chairman K, Mathew KE, Padmalatha C, Ranjit AJ. Beware of pathogenic microbes in public utility devices. J Microbiol Biotechnol Res. 2011;1(3):85-90.
[14] Klevens RM, Edwards JR, Richards CL Jr, Horan TC, Gaynes RP, Pollock DA, Cardo DM. Estimating health care-associated infections and deaths in U.S. hospitals, 2002. Public Health Rep. 2007 Mar-Apr;122(2):160-6. DOI: 10.1046/j.1365-2672.2002.01734.x
[15] Rusin P, Maxwell S, Gerba C. Comparative surface-to-hand and fingertip-to-mouth transfer efficiency of gram-positive bacteria, gram-negative bacteria, and phage. J Appl Microbiol. 2002;93(4):585-92. DOI: 10.1046/j.1365-2672.2002.01734.x
[16] Mahon CR, Manuselis G Jr, eds. Textbook of Diagnostic Microbiology. Philadelphia: Saunders; 1995.
[17] Mahmoudi H, Arabestani MR, Mousavi SF, Alikhani MY. Molecular analysis of the coagulase gene in clinical and nasal carrier isolates of methicillin-resistant Staphylococcus aureus by restriction fragment length polymorphism. J Glob Antimicrob Resist. 2016 Dec;8:41-45. DOI: 10.1016/j.jgar.2016.10.007
[18] Karabay O, Kooglu E, Tahtaci M. The role of mobile phones in the spread of bacteria associated with nosocomial infections. J Infect Dev Ctries. 2007;1:72-3.
[19] Ferdinandus J, Hensckhe K, Palombo EA. Isolation of pathogenic bacteria and opportunistic pathogens from public telephones. Environmental Health. 2001;1(2): 74-9.
[20] Marcham CL. Coats, ties, stethoscopes, cell phones, and id badges: Potential source of healthcare-associated infections. Univ Oklahoma Environm Health Safety Office, Safe T Gram. 2009;16(1):1-3. Available from: http://compliance.ouhsc.edu/LinkClick.aspx?fileticket=sKtRl7RFrvo%3D&portalid=71
[21] Neely AN, Maley MP. Survival of enterococci and staphylococci on hospital fabrics and plastic. J Clin Microbiol. 2000 Feb;38(2):724-6.
[22] Ramesh J, Carter AO, Campbell MH, Gibbons N, Powlett C, Moseley H Sr, Lewis D, Carter T. Use of mobile phones by medical staff at Queen Elizabeth Hospital, Barbados: evidence for both benefit and harm. J Hosp Infect. 2008 Oct;70(2):160-5. DOI: 10.1016/j.jhin.2008.06.007
[23] Ashgar SS, El-Said HM. Pathogenic bacteria associated with different public Environmental sites in Mecca city. Open J Med Microbiol. 2012;2(04):133-7. DOI: 10.4236/ojmm.2012.24020
[24] Malik K, Naeem N. Study of bacteria on computer's mice and keyboards. Int J Curr Microbiol App Sci. 2014;3(4):813-23.
[25] Oluduro AO, Ubani A, Ofoezie I. Bacterial assessment of electronic hardware user interfaces in Ile-ife, Nigeria. Rev Ciênc Farm Básica Apl. 2012;32(3):323-34.
[26] Yazah A, Yusuf J, Agbo A. Bacterial contaminants of Nigerian currency notes and associated risk factors. Res J Med Sci. 2012;6(1):1-6. DOI: 10.3923/rjmsci.2012.1.6
[27] Cataño JC, Echeverri LM, Szela C. Bacterial contamination of clothes and environmental items in a third-level hospital in Colombia. Interdiscip Perspect Infect Dis. 2012;2012:507640. DOI: 10.1155/2012/507640
[28] Onuoha SC, Fatokun K. Bacterial contamination and public health risk associated with the use of banks' automated teller machines (atms) in Ebonyi State, Nigeria. Amer J Publ Health Res. 2014;2(2):46-50. DOI: 10.12691/ajphr-2-2-2
[29] Fazeli H, Akbari R, Moghim S, Narimani T, Arabestani MR, Ghoddousi AR. Pseudomonas aeruginosa infections in patients, hospital means, and personnel's specimens. J Res Med Sci. 2012 Apr;17(4):332-7.
[30] Nworie O, Mercy M, Chukwudi A, Oko I, Chukwudum SO, Agah VM, Ekuma UO. Antibiogram of bacteria isolated from automated teller machines within abakaliki metropolis. Am J Inf Dis. 2012;8(4):168-74. DOI: 10.3844/ajidsp.2012.168.174
[31] Hübner NO, Hübner C, Wodny M, Kampf G, Kramer A. Effectiveness of alcohol-based hand disinfectants in a public administration: impact on health and work performance related to acute respiratory symptoms and diarrhoea. BMC Infect Dis. 2010 Aug;10:250. DOI: 10.1186/1471-2334-10-250

