Results after simple decompression of the ulnar nerve in cubital tunnel syndrome
Kristina Harder 1,2Sandra Lukschu 1,2
Sebastian E. Dunda 1,2
Björn Dirk Krapohl 1,2
1 Department of Plastic and Hand Surgery, St. Marien-Krankenhaus Berlin, Germany
2 Center for Musculoskeletal Surgery, Charité – Medical University of Berlin, Germany
Abstract
Cubital tunnel syndrome represents the second most common compression neuropathy of the upper limb. For more than four decades there has been a controversy about the best surgical treatment modality for cubital tunnel syndrome.
In this study the results of 28 patients with simple ulnar nerve decompression are presented. Data analyses refers to clinical examination, personal interview, DASH-questionnaire, and electrophysiological measurements, which were assessed pre- and postoperatively.
28 patients (15 females, 13 males) were included in this study. The average age at time of surgery was 47.78 years (31.68–73.10 years). The period from onset of symptoms to surgery ranged from 2 to 24 months (mean 6 months). The mean follow-up was 2.11 years (0.91–4.16 years).
Postoperatively there was a significant decrease in DASH score from 52.6 points to 13.3 points (p<0.001). Also the electrophysiological findings improved significantly: motor nerve conduction velocity increased from 36.0 m/s to 44.4 m/s (p=0.008) and the motor nerve action potential reached 5,470 mV compared to 3,665 mV preoperatively (p=0.018). A significant increase of grip strength from 59% (in comparison to the healthy hand) to 80% was observed (p=0.002). Pain was indicated by means of a visual analog scale from 0 to 100. Preoperatively the median level of pain was 29 and postoperatively it was 0 (p=0.001). The decrease of the two-point-discrimination of the three ulnar finger nerves was also highly significant (p<0.001) from 11.3 mm to 5.0 mm. Significant postoperative improvement was also observed in the clinical examination concerning muscle atrophy (p=0.002), clawing (p=0.008), paresthesia (p=0.004), the sign of Froment (p=0.004), the sign of Hoffmann-Tinel (p=0.021), and clumsiness (p=0.002).
Overall nearly 90% of all patients were satisfied with the result of the operation. In 96.4% of all cases, surgery improved the symptoms and in one patient (3.6%) the success was noted as “poor” because the symptoms remained unchanged. In 35.7% the success was graded as “moderate”, in 10.7% as “good” and in 50.0% as “very good”.
Keywords
cubital tunnel syndrome, nerve decompression, DASH score
Introduction
The cubital tunnel syndrome (CTS) is a frequent diagnosis for neuropathy of the upper limb. It is characterized by pain at the ulnar part of the forearm, paresthesia, and hypesthesia, accompanied by sensitive and motoric dysfunction. This leads to a severe disability and restrictions in daily life.
There are multiple treatment options concerning surgical interventions but still without an academic level of evidence for one of them.
The investigators of this study present a long-term follow-up with a complex clinical and physiological testing scale after single decompression of the ulnar nerve in cubital tunnel syndrome.
Methods and material
During a three year period 56 single decompression operations caused by cubital tunnel syndrome were performed in the institution. 28 patients could be randomized into the study. The mean follow-up was 2.1 years after operation and was realized by an extensive protocol of examinations. The patients were evaluated by a questionnaire, including the DASH score, visual analogue scale, and a general assessment on the subjective benefit of the operation and its effect.
Furthermore, we examined the patients focusing on the parameters: grip strength (Jamar dynamometer), range of motion, functional thumb adduction (Froment sign), static two point discrimination, nerve irritation (Hoffmann-Tinel sign), and electroneurophysiological parameters.
Results
There was an equal distribution of sex (53.6% female, 46.4% male). The mean age was 48 years and the persistence of symptoms until operation was 6 months (2–24). Remarkable was the affliction of the non-dominant hand:
The DASH score (Disability of the arm, shoulder and hand) was significantly reduced post-operatively (52.6 vs. 13.3; p<0.001) as well as the pain-scale and the feeling of clumsiness of the hand. Preoperatively the median level of pain was 29 and postoperatively it was 0 (p=0.001).
Concerning the technical examination grip strength measured by Jamar dynamometer showed an improvement. A significant increase of grip strength from 59% (in comparison to the healthy hand) to 80% was observed (p=0.002). Pain was indicated by means of a visual analog scale from 0 to 100. Preoperatively the median level of pain was 29 and postoperatively it was 0 (p=0.000). The decrease of the two-point-discrimination of the three ulnar finger nerves was also highly significant (p<0.001) from 11.3 mm to 5.0 mm. Significant postoperative improvement was also observed in the clinical examination concerning muscle atrophy (p=0.002), clawing (p=0.008), paresthesia (p=0.004), the sign of Froment (p=0.004), the sign of Hoffmann-Tinel (p=0.021), and clumsiness (p=0.002). Overall nearly 90% of all patients were satisfied with the result of the operation. In 96.4% of all cases, surgery improved the symptoms and in one patient (3.6%) the success was noted as “poor” because the symptoms remained unchanged. In 35.7% the success was graded as “moderate”, in 10.7% as “good” and in 50.0% as “very good” (Figure 1 [Fig. 1]).
Figure 1: Patients’ rating of the result after nerve decompression in cubital tunnel syndrome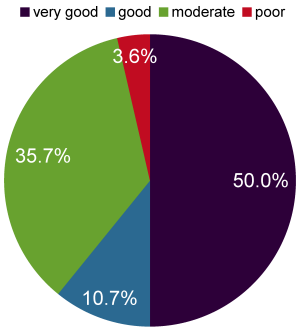
Paraesthesia is one of the major symptoms and were found in 27 from 28 patients before the operation. This was also reduced significantly (p=0.004) by the operation, but 18 patients reported about any kind of paraesthetic feelings.
Also the positive Hofmann-Tinel sign was persisting in 12 of 21 cases.
The most important parameters, DASH score, pain scale, and grip strength are summarized in Figure 2 [Fig. 2].
Figure 2: Summary of the most important parameters, comparing the state before and after ulnar nerve decompression in cubital tunnel syndrome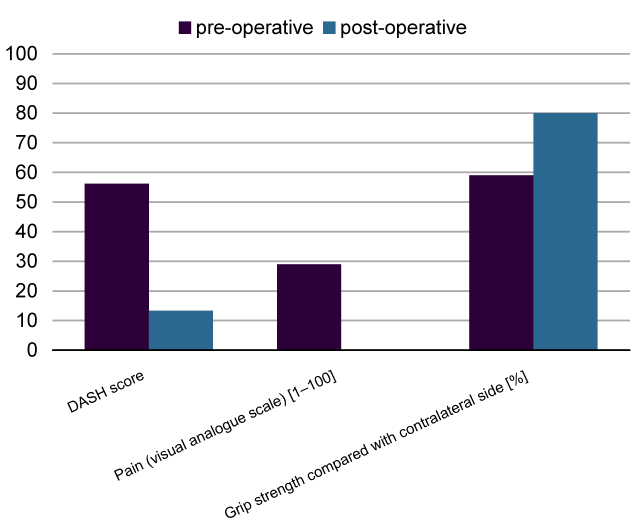
Discussion
Even in the 21st century, there are multiple uncertainties in diagnostic and treatment methods of cubital tunnel syndrome. Up to 30% of patients suffering from cubital tunnel syndrome are idiopathic and then often correlated with an additional carpal tunnel syndrome. The diagnostics even in case of neurophysiological testing do not necessarily correlate with the clinical findings and symptoms [1]. The benefit of the operation is reduction of pain, increase of motor und sensory function of the inflicted arm. The standard methods for surgery include simple nerve-decompression, different types of transposition of the ulnar nerve, and medial epicondylectomy. However, there is no evidence for any of them to deliver significantly better results than one of the other techniques [2], [3], [4].
There are multiple investigations concerning the treatment of the cubital tunnel syndrome but only rare studies are randomized or prospectively planned [5].
The single nerve decompression, open or endoscopically, is the operation with the lowest tissue trauma and the fewest damage to the Vasa nervorum [6], [7]. The transposition of the nerve is more complex and gets along with a higher incidence of peri-operative complications [3].
This study confirms the excellent outcome after single decompression of the ulnar nerve. The investigators propose this method as „gold standard“ in cases of cubital tunnel syndrome without anatomical pathologies that require further manipulation.
Conclusion
The single ulnar nerve decompression is a safe and effective method to treat the cubital tunnel syndrome. It achieves significantly a reduction of pain and paresthesia, an increase of power and the motoric and sensitive function.
Notes
Competing interests
The authors declare that they have no competing interests.
References
[1] Tomaino MM, Brach PJ, Vansickle DP. The rationale for and efficacy of surgical intervention for electrodiagnostic-negative cubital tunnel syndrome. J Hand Surg Am. 2001 Nov;26(6):1077-81. DOI: 10.1053/jhsu.2001.26327[2] Gervasio O, Gambardella G, Zaccone C, Branca D. Simple decompression versus anterior submuscular transposition of the ulnar nerve in severe cubital tunnel syndrome: a prospective randomized study. Neurosurgery. 2005;56(1):108-17; discussion 117.
[3] Nabhan A, Kelm J, Steudel WI, Shariat K, Sova L, Ahlhelm F. Sulcus-ulnaris-Syndrom: Einfache Dekompression oder subkutane Vorverlagerung [Cubital tunnel syndrome--simple nerve decompression or decompression with subcutaneous anterior transposition?]. Fortschr Neurol Psychiatr. 2007 Mar;75(3):168-71. DOI: 10.1055/s-2006-955004
[4] Kim KW, Lee HJ, Rhee SH, Baek GH. Minimal epicondylectomy improves neurologic deficits in moderate to severe cubital tunnel syndrome. Clin Orthop Relat Res. 2012 May;470(5):1405-13. DOI: 10.1007/s11999-012-2263-1
[5] Bartels RH, Verhagen WI, van der Wilt GJ, Meulstee J, van Rossum LG, Grotenhuis JA. Prospective randomized controlled study comparing simple decompression versus anterior subcutaneous transposition for idiopathic neuropathy of the ulnar nerve at the elbow: Part 1. Neurosurgery. 2005 Mar;56(3):522-30. DOI: 10.1227/01.NEU.0000154131.01167.03
[6] Huang JH, Samadani U, Zager EL. Ulnar nerve entrapment neuropathy at the elbow: simple decompression. Neurosurgery. 2004 Nov;55(5):1150-3. DOI: 10.1227/01.NEU.0000140841.28007.F2
[7] Bultmann C, Hoffmann R. Die endoskopische Dekompression des Nervus ulnaris bei Kubitaltunnelsyndrom [Endoscopic decompression of the ulnar nerve in cubital tunnel syndrome]. Oper Orthop Traumatol. 2009 Jun;21(2):193-205. DOI: 10.1007/s00064-009-1707-6

