The potential of the individualized treatment with the new cochlear implant electrode array FLEX34
Daniel Polterauer 1,2Andrea Schreier 1,2
Carmen Molenda 1,2
Sarah Draut 1,2
Maike Neuling 1,2
John Martin Hempel 1,2
Joachim Müller 1,2
1 Department of Otorhinolaryngology, Head & Neck Surgery, LMU Munich, Germany
2 Section Otology and Cochlear Implants, LMU Munich, Germany
Abstract
Using fine-slice imaging (CT, MRI), it is now possible to determine the cochlear length (CDL) preoperatively to cochlear implantation. This allows for individualized cochlear implant implantation adapted to the individual anatomy. Electrode arrays can be inserted virtually using the OTOPLAN4 software (CAScination, Bern, Switzerland; distributed by MED-EL, Innsbruck, Austria). The aim was to investigate how often a particularly long cochlea is present and therefore implantation of the currently longest electrode array, FLEX34, would have been possible. We examined all CI patients in our database with CDL measured via OTOPLAN4 based on the full organ of corti (CDL (full OC)) retrospectively. OTOPLAN4 also allows automatic evaluation in contrast to previous versions. To calculate the potential coverage of a FLEX34, it was assumed according to the manufacturer’s instructions that the apical electrode was at a position of 33.62 mm CDL (full OC). The CDL (full OC) and the electrical cochlear coverage were compared. A total of 196 ears from 99 patients were analyzed with OTOPLAN4. The A value was 9.24±0.80 mm from 7.7 to 15 mm, the average H value was 4.12±0.43 mm from 3.0 to 5.4 mm, the B value was 6.83±0.57 mm from 3.9 to 8.4 mm and the CDL (full OC) at 36.13±2.48 mm from 30.4 to 46.4 mm (each arithmetic mean ± SD from min. to max.). Mean electrical cochlear coverage was 93.04±6.65% from 70.89% to 111.14%. In 28 cases (14.29%) the coverage was ≥100%, in 115 cases (58.67%) 90–100%, in 45 cases (22.96%) 80–90%, and in 7 cases (3.57%) 70–80%. To conclude, at our clinic, a significant proportion of patients have a very large cochlea and would potentially benefit from an even longer electrode such as the FLEX34 resulting in a higher cochlear coverage. Which cochlear coverage should be aimed for individually needs to be examined in more detail in further studies, as there is currently data that recommend around 80% coverage as well as data that suggest the most complete coverage possible to achieve the best possible speech understanding postoperatively.
Keywords
individualized cochlear implantation, FLEX34, cochlear duct length, OTOPLAN
Introduction
In cochlear implantation, choosing the ideal electrode for each patient is crucial. The electrode arrays have gone through several conceptual changes during the past decades and as we have entered the era of personalized medicine there is a shift towards a more individualized cochlear implantation and focusing even more on the individual patient characteristics. Considering the individual cochlear anatomy is a central step in the electrode array election. It has been shown that there is a broad variation in the morphology of the cochlea, which can be estimated via the cochlea duct length (CDL) [1]. To serve this variety of cochleae different electrode arrays are needed. Especially for very long cochleae (CDL≥38 mm) there are limited options available with the longest electrode measuring 31 mm [2]. In comparison, the 31 mm straight electrode arrays of MED-EL are longer than electrode arrays from other CI manufacturers. To meet this need, an even longer electrode array was designed, the FLEX34 [3], [4], with a total length of 34 mm. Electrode selection depends on various factors like hearing preservation and anatomical anomalies [5], [6], [7]. However, several studies have revealed certain benefits of long electrodes [1], [8], [9], [10], including better speech understanding in quiet and noise, possibly resulting from a higher cochlear coverage and therefore better tonotopic mapping. Using fine-slice imaging (CT, MRI), it is now possible to determine the CDL preoperatively. This allows for individualized cochlear implant implantation adapted to the individual anatomy. Electrode arrays can be inserted virtually using the OTOPLAN4 software (CAScination, Bern, Switzerland; distributed by MED-EL, Innsbruck, Austria). The current study aimed to investigate how often a particularly long cochlea is present and therefore implantation of the currently longest electrode array, FLEX34, would have been possible.
Methods and results
We examined all CI patients in our database with CDL measured via OTOPLAN4 based on the full organ of corti (CDL (full OC)) retrospectively. OTOPLAN4 also allows automatic evaluation in contrast to previous versions. To calculate the potential coverage of a FLEX34, it was assumed – according to the manufacturer’s instructions – that the apical electrode was at a position of 33.62 mm CDL (full OC). We compared the CDL (full OC) and the electrical cochlear coverage.
We analyzed 196 ears from 99 patients with OTOPLAN4. The A value was 9.24±0.80 mm from 7.7 to 15 mm, the average H value was 4.12±0.43mm from 3.0 to 5.4 mm, the B value was 6.83±0.57 mm from 3.9 to 8.4 mm and the CDL (full OC) at 36.13±2.48 mm from 30.4 to 46.4 mm (each arithmetic mean ± SD), see Figure 1 [Fig. 1] and Figure 2 [Fig. 2]. Mean electrical cochlear coverage was 93.04±6.65% from 70.89% to 111.14%. In 28 cases (14.29%) the coverage was ≥100%, in 115 cases (58.67%) 90–100%, in 45 cases (22.96%) 80–90%, and in 7 cases (3.57%) 70–80%. The distribution of the cochlear coverage estimated by OTOPLAN is visualized in Figure 3 [Fig. 3]. For cochleae with an electrical coverage of ≥100% the FLEX34 seems too long based on the OTOPLAN estimation’s results. In 35 cases (17.86%), the CDL (full OC) was ≥38.00 mm, which can be used, for example, as a cut-off value for the implantation of a FLEX34. In three cases (1.53%), a FLEX34 was implanted.
Figure 1: Grouped CDL frequency distribution in the examined patient population in mm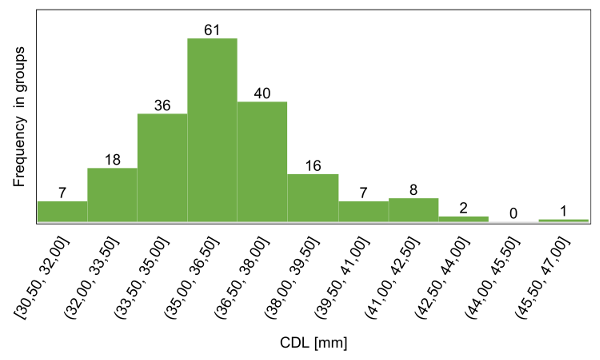
Figure 2: Average cochlear parameters in the examined patient group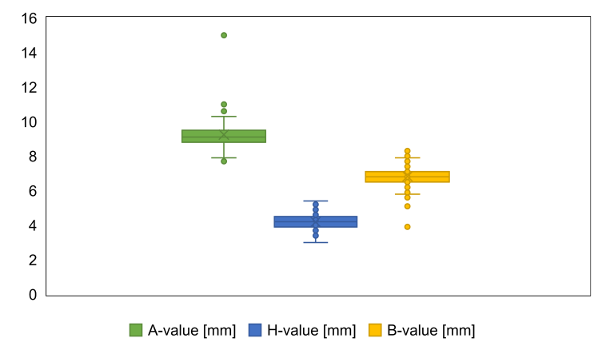
Figure 3: Grouped frequency distribution of electric coverage estimated through preoperative imaging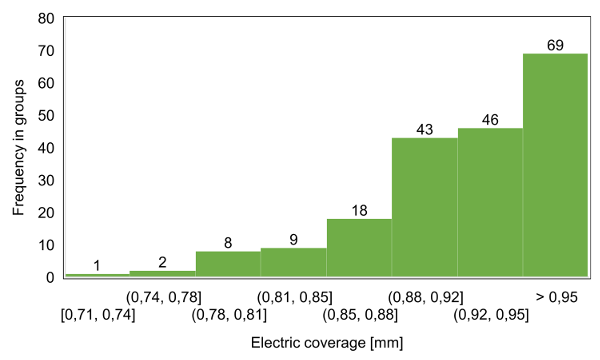
Discussion
The study aimed to investigate the potential application of the currently longest electrode array, FLEX 34. For this purpose, it was examined how often a very long cochlea is present using a new surgical planning software, OTOPLAN4, and thus implantation of the FLEX34 would have been possible. The hypothesis here was that there is a great application potential for longer electrode arrays such as the FLEX34. Therefore, a relevant proportion of patients with a longer CDL would need a longer electrode to reach the same and sufficient cochlear coverage. This way, they could benefit from better tonotopic matching. Several studies have shown that there is a broad range of individual CDL, ranging from 25–45 mm [11], [12], [13].
In this study, we found a relevant proportion of patients with a larger cochlear duct. These patients could benefit from a longer electrode array, specifically the FLEX34. If all patients we examined would have been implanted with a FLEX34, then around 23% would have had a cochlear coverage between 80–90% and around 3.5% between 70–80%.
In N=196 ears, we found a mean CDL of around 36 mm, which is also consistent with the literature [11], [12], [13]. Regarding the ideal cochlear coverage, the research is still ongoing. Alothman et al. reported a significantly better speech discrimination score in children with cochlear coverage >82,78% than those with a coverage <82,78% [14]. Weller et al. found that patients with a cochlear coverage between 79–82% obtained better postoperative word recognition scores than patients with a cochlear coverage <70%, however, results indicated that patients with a cochlear coverage >82% may not profit from an additional benefit [15]. Although further studies are needed, the recommended cochlear coverage of around 80% could be reached by roundabout 27% of our patients when being implanted with a FLEX34 (cochlear coverage between 70–90%). However, only in 1.5% of the cases, there was a FLEX34 implanted. On one hand, there are cochleae that got too short CDL for a FLEX34 electrode array (>100% electrical coverage). On the other hand, there is a high percentage of patients, which could receive a FLEX34 instead of shorter arrays. This group size may vary depending on the upper limit for electrical coverage set by individual surgeons due to a lack of national consensus. Especially, when an electrical coverage of around 90% or even higher is accepted, clinical applications will find a large number of FLEX34 candidates. Therefore, there is a great potential for the provision of longer electrodes in terms of individualized cochlear implantation to achieve higher cochlear coverage and thus potentially a better outcome. Eventually, this is also the basis for anatomy-based fitting, another step towards a more precise and personalized cochlear implantation.
The study has a few limitations. Firstly, we have a limited number of patients. However, when looking at the literature, we have a comparable amount, and, on the other hand, this was the first evaluation of the applicability of a comparably long electrode. Secondly, it is a retrospective study design, but then again, this was an early study to evaluate the potential. Thirdly, CDL was measured and estimated via the software OTOPLAN4 and might show slight deviations from other methods. Nevertheless, this is the latest version with an automatic and therefore reproducible evaluation that has been an established method so far.
To conclude, at our clinic, a significant proportion of patients have a very large cochlea and would potentially benefit from a long electrode array such as the FLEX34 resulting in a higher cochlear coverage. Which cochlear coverage should be aimed for individually needs to be examined in more detail in further studies, as there is currently data that recommend around 80% coverage as well as data that suggest the most complete coverage possible to achieve the best possible speech understanding postoperatively.
Notes
Conference presentation
This contribution was presented at the 26th Annual Conference of the German Society of Audiology and published as an abstract [16].
Ethics statement
Institutional Review Board Statement: The LMU Review Board, protocol number 17-227, approved this study.
Competing interests
The authors declare that they have no competing interests.
References
[1] Hochmair I, Hochmair E, Nopp P, Waller M, Jolly C. Deep electrode insertion and sound coding in cochlear implants. Hear Res. 2015 Apr;322:14-23. DOI: 10.1016/j.heares.2014.10.006[2] Dhanasingh A, Hochmair I. Special electrodes for demanding cochlear conditions. Acta Otolaryngol. 2021 Mar;141(sup1):157-77. DOI: 10.1080/00016489.2021.1888506
[3] Müller J. Deep Electrode Insertion in Cochlear Implants: Apical morphology, Electrode and Inital Speech Perception Results of a New 34mm Electrode. In: CI2016 14th International Conference on Cochlear Implants; 2016 May 11-14; Toronto.
[4] Schreier A, Molenda C, Draut S, Hempel JM, Volgger V, Polterauer D, Merz L, Müller J . Individualized cochlear implantation - a new, longer electrode array to meet the need for patients with very long cochleae: first experience with a new 34 mm electrode. Laryngorhinootologie. 2024; 103(S 02):S269. DOI: 10.1055/s-0044-1784895
[5] Müller J, Molenda C, Polterauer D. Aktuelle Trends und Entwicklungen bei der Cochlea-Implantat-Versorgung [Current Trends and Developments in Cochlear Implantation]. Sprache Stimme Gehör. 2024;48(01):22-31. DOI: 10.1055/a-2195-4886
[6] Dillon MT, Buss E, O'Connell BP, Rooth MA, King ER, Bucker AL, Deres EJ, McCarthy SA, Pillsbury HC, Brown KD. Low-Frequency Hearing Preservation With Long Electrode Arrays: Inclusion of Unaided Hearing Threshold Assessment in the Postoperative Test Battery. Am J Audiol. 2020 Mar;29(1):1-5. DOI: 10.1044/2019_AJA-19-00045
[7] Polterauer D, Molenda C, Neuling M, Hempel J-M, Müller J. Pre-operative anatomical analysis estimating optimal electrode array in Cochlear Implant candidates based on CT or MRI images. Laryngorhinootologie. 2024;103(S02):S264-5. DOI: 10.1055/s-0044-1784879
[8] Canfarotta MW, Dillon MT, Brown KD, Pillsbury HC, Dedmon MM, O'Connell BP. Insertion Depth and Cochlear Implant Speech Recognition Outcomes: A Comparative Study of 28- and 31.5-mm Lateral Wall Arrays. Otol Neurotol. 2022 Feb;43(2):183-9. DOI: 10.1097/MAO.0000000000003416
[9] Canfarotta MW, Dillon MT, Buss E, Pillsbury HC, Brown KD, O'Connell BP. Frequency-to-Place Mismatch: Characterizing Variability and the Influence on Speech Perception Outcomes in Cochlear Implant Recipients. Ear Hear. 2020;41(5):1349-61. DOI: 10.1097/AUD.0000000000000864
[10] Dillon MT, Canfarotta MW, Buss E, O'Connell BP. Comparison of Speech Recognition With an Organ of Corti Versus Spiral Ganglion Frequency-to-Place Function in Place-Based Mapping of Cochlear Implant and Electric-Acoustic Stimulation Devices. Otol Neurotol. 2021 Jun;42(5):721-25. DOI: 10.1097/MAO.0000000000003070
[11] Lee J, Nadol JB Jr, Eddington DK. Depth of electrode insertion and postoperative performance in humans with cochlear implants: a histopathologic study. Audiol Neurootol. 2010;15(5):323-31. DOI: 10.1159/000289571
[12] Spiegel JL, Polterauer D, Hempel JM, Canis M, Spiro JE, Müller J. Variation of the cochlear anatomy and cochlea duct length: analysis with a new tablet-based software. Eur Arch Otorhinolaryngol. 2022 Apr;279(4):1851-61. DOI: 10.1007/s00405-021-06889-0
[13] Timm ME, Majdani O, Weller T, Windeler M, Lenarz T, Büchner A, Salcher RB. Patient specific selection of lateral wall cochlear implant electrodes based on anatomical indication ranges. PLoS One. 2018;13(10):e0206435. DOI: 10.1371/journal.pone.0206435
[14] Alothman N, Almuhawas F, Badghaish R, Alotaibi AH, Alhabib SF, Alzhrani F, Hagr A. Cochlear Implantation in Pediatrics: The Effect of Cochlear Coverage. J Pers Med. 2023 Mar;13(3):562. DOI: 10.3390/jpm13030562
[15] Weller T, Timm ME, Lenarz T, Büchner A. Cochlear coverage with lateral wall cochlear implant electrode arrays affects post-operative speech recognition. PLoS One. 2023;18(7):e0287450. DOI: 10.1371/journal.pone.0287450
[16] Polterauer D, Schreier A, Molenda C, Draut S, Neuling M, Hempel JM, Müller J. Potential der individualisierten Versorgung mit dem neuen CI-Elektrodenträger FLEX34. In: Deutsche Gesellschaft für Audiologie e.V., editor. 26. Jahrestagung der Deutschen Gesellschaft für Audiologie; Aalen, 06.-08.03.2024. Düsseldorf: German Medical Science GMS Publishing House; 2024. Doc141. DOI: 10.3205/24dga141

