[Randomisierte Cross-Over-Bewertung vom Geschlecht des Untersuchers auf die Schmerzschwelle bei gesunden Freiwilligen]
Anna Sellgren Engskov 1Ilja Lejbman 1
Jonas Åkeson 1
1 Department of Clinical Sciences Malmö, Anaesthesiology and Intensive Care Medicine, Lund University, Malmö, Sweden
Zusammenfassung
Hintergrund und Ziele: Diese präklinische randomisierte Cross-Over-Studie wurde entwickelt, um 1) einen möglichen Einfluss des Geschlechts der Untersucher auf die Schwellenwerte für elektrische Schmerzen (EPT) und entsprechende Schmerzintensität bei gesunden Freiwilligen zu bewerten, und 2) mögliche Unterschiede bei diesen Interventionen zwischen weiblichen und männlichen Studienteilnehmern zu bewerten.
Methoden: Vierzig gesunde erwachsene Freiwillige (22 Frauen) wurden eingeschlossen. Mit einem elektrischen Stimulationsgerät wurden die EPT-Spiegel in Dreierreihen bei jedem Studienteilnehmer – einmal von einem weiblichen und einmal von einem männlichen Untersucher – gemäß einem vordefinierten Cross-Over-Entwurfsplan bestimmt. Entsprechende Niveaus der Schmerzintensität wurden auf einem VAS-Lineal bewertet.
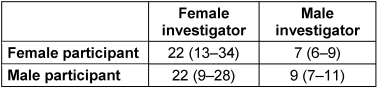
Ergebnisse: Studiendaten wurden bei allen Teilnehmern erhoben und analysiert. Im Vergleich zum männlichen Untersucher wurden von der weiblichen Untersucherin signifikant höhere EPT-Spiegel bestimmt (Median 22 (IQR 12–31) vs. 8 (6–10) Schmerzstärkeneinheiten; p<0,0001)), trotz ähnlicher Niveaus der berichteten Schmerzintensität (1,9 (1,2–3,0) vs. 2,0 (1,1–3,4) VAS-Einheiten; p>0,300). Es gab keine Unterschiede in EPT zwischen weiblichen und männlichen Teilnehmern, die von weiblichen (p>0,300) und männlichen (p=0,125) Untersuchern bewertet wurden, oder zwischen der ersten und zweiten Stimulationsreihe (p>0,300).
Schlussfolgerungen: Dass signifikant höhere EPT-Werte bei Studienteilnehmern beiden Geschlechts vorlagen, wenn sie von einer weiblichen statt einer männlichen Person untersucht wurden – trotz gleicher gemeldeter Schmerzintensität –, zeigt einen möglichen Einfluss des Geschlechts des Untersuchers auf die individuelle Wahrnehmung von Schmerz.
Implikationen: Durch diesen Beitrag zu einem besseren Verständnis, wie die individuellen EPT-Werte möglicherweise vom Geschlecht des Untersuchers beeinflusst werden, könnte diese Studie die zukünftige Bewertung von Schmerzzuständen sowohl im präklinischen als auch im klinischen Umfeld erleichtern.
Introduction
Individual perception of pain is generally believed to be influenced by both physiological and psychosocial factors. The biological term ‘sex’ and the social term ‘gender’ (according to definitions by the World Health Organization) have both been proposed to be important regarding study participants [1] as well as investigators [2] in this context. To reflect how they are frequently being perceived, the term ‘gender’ is mainly used in this study.
Pain threshold is the level where extreme temperatures and pressures (or injury-related chemicals) activate nociceptors, i.e. peripheral sensory neurons, with following transduction and processing of stimuli in higher brain centres, resulting in pain perception [3].
Evaluations by female investigators have been associated with higher thresholds of pain induced by mechanical pressure [4] or laser [5] stimulation, and with lower intensity of pain induced by heat [6] or cold [7] stimulation in study participants. However, female investigators have also been reported to obtain similar levels of pain threshold, but lower levels of pain tolerance to cold-induced nociceptive stimulation [8]. Higher warm and cool thresholds, but not heat and cold pain thresholds, have been found in subjects evaluated by investigators of opposite gender [9]. The influence of investigator gender on pain perception after heat stimulation has been reported not to be associated with corresponding physiological changes in heart rate [6], possibly reflecting perceived traditional gender roles [4], [7], [9].
Numerous original studies on subject gender with different pain stimuli have found lower pain threshold levels [8], [10], [11], [12], [13], [14], [15], [16], [17], [18], [19], [20] or higher pain intensity levels [7], [21], [22], [23] in females – recently confirmed in two reviews [1], [24], possibly reflecting physiological sex differences [21] or psychosocial factors [25] like gender-role expectations [26], [27] – whereas others have found no differences [5], [9], [13], [27], [28].
Based on available data in females and males evaluated by investigators of both genders [4], [5], [7], [17], [23], our main study hypothesis was that evaluations by female investigators result in higher pain threshold levels and/or lower pain intensity levels than evaluations by male investigators. Our second study hypothesis was that females have lower pain threshold levels and/or report higher pain intensity levels than males regardless of investigator gender.
This randomized paired cross-over study was designed to evaluate potential impact of the gender of study investigators and participants on electrical pain threshold (EPT) levels and pain intensity levels.
Subjects and methods
Study setting
This prospective randomized paired cross-over study in adult healthy volunteers, approved by the regional Human Research Ethics Review Board (Approval No. 2015/779), Lund, and carried out in May 2016 at Skåne University Hospital, Malmö, Sweden, was designed to evaluate and compare EPT levels and individually scored pain intensity levels in study participants of both genders.
Each participant was evaluated twice, at 10-to-15-minute intervals during daytime, according to a predefined randomized cross-over design schedule, by a 36-year-old female and a 27-year-old male resident in anaesthesiology and intensive care medicine with similar BMI and external appearance. The investigators, dressed in white physician coats, provided identical study information by reading a defined text from a paper in a private and quiet room. They knew the main purpose of the study.
Subjects
Forty healthy adult volunteers (22 females) with normal health declaration and no current history of pain, use of analgesics, or use of other drugs affecting pain perception, were included after normal physical examination and individual verbal and written informed consent. Extensive physical activity within twelve hours and use of analgesic or alcohol within 24 hours before the study sessions were not allowed. All subjects were informed in advance by e-mail that their pain thresholds were to be determined twice with an established device designed for that specific purpose, but no instructions were given on how to use it. They were not informed about the main purpose of the study – evaluating potential influence of investigator and participant gender on pain perception – until after having participated.
Induction of pain
In each study participant, pain was then induced in two series (at least ten minutes apart) of three stimulations with an electrical stimulation device (Painmatcher®, Cefar Medical AB, Lund, Sweden), delivering rectangular electrical pulses of 10 Hz frequency and 15 mA amplitude. Each subject was told to close an electrical circuit – to gradually increase the pulse duration stepwise by 4 µs – by pressing two buttons on the device between their right thumb and index finger pulps, and then to release the buttons as soon as the level of stimulation was considered to be painful, i.e. defined to correspond to their individual EPT, measured in pain magnitude scores (0–99), on a hidden display. The design of the device makes it involve the same parts of the fingers during all stimulations in each individual. Two identical devices, calibrated immediately before the study period by the Department of Medical Techniques, Skåne University Hospital, Malmö, Sweden, were used. Each device was used by each investigator in half of the study participants.
Evaluation of pain
Immediately after each series of three stimulations, the maximum intensity at pain threshold was scored by the participant, according to established principles, on a horizontal visual analog scale (VAS) slide ruler, and subsequently handed over for the investigator to record the score from the back side with one decimal.
Statistics
The influence of investigator gender on individually reported levels of pain intensity has previously been confirmed in 64 volunteer participants, subjected to experimental thermal pain and evaluated by VAS scoring with an unpaired study design [6]. Based on those findings, 40 study participants were estimated to be enough for evaluation of electrical pain thresholds in the present study, taking up to 20 percent potential dropouts into account. This number of participants was calculated to enable a difference of 6±12 pain magnitude scores between evaluations by female and male investigators to be confirmed with 80% statistical power and 95% statistical probability, based on paired cross-over comparison.
Individual EPT levels were calculated as average values of the three EPT values recorded in each series of stimulation. The Wilcoxon signed rank test was used to compare EPT levels and corresponding pain intensity score levels in study participants evaluated by female and male investigators, and to evaluate potential order and carry-over effects by comparing pain responses to the first and second series of stimulation. The Mann-Whitney U-test was used to compare EPT levels and pain intensity score levels between female and male subjects.
Parametric data is reported as mean ± standard deviation (SD), and non-parametric data as median with interquartile range (IQR) in parenthesis.
Levels of probability (p) below 0.01 were considered to reflect statistical significance to enable up to five multiple tests.
Results
Subjects
Results were obtained and analysed in 40 (22 female) 26±4-year-old subjects with a body weight of 68±11 kg and a body height of 175±10 cm.
Induction of pain
Each study participant followed the verbal instructions carefully and perceived the pain task accordingly, once with the female and once with the male investigator.
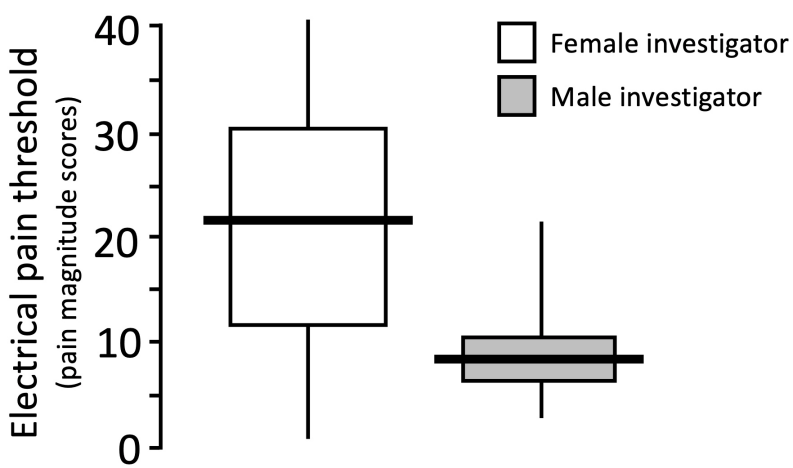
Individually calculated EPT levels were significantly higher (p<0.0001) when obtained by the female (median 22 (IQR 12–31) pain magnitude scores) than by the male (8 (6–10) pain magnitude scores) investigator (Figure 1 [Fig. 1]), and were higher in 33 evaluations (82%) made by the female. The EPT levels did not differ between female and male subjects evaluated by female (p>0.300) or male (p=0.125) investigators (Table 1 [Tab. 1]), or between the first and second series of stimulation (11 (7–19) vs. 11 (6–22) pain magnitude scores; p>0.300).
Evaluation of pain
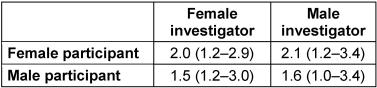
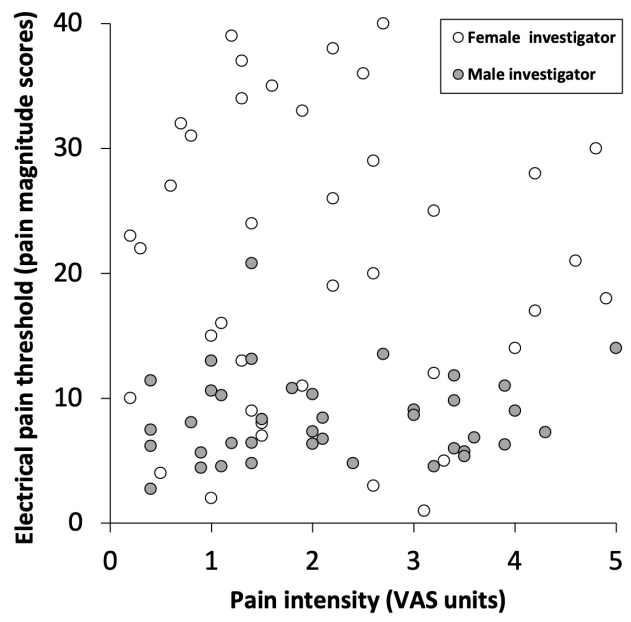
As shown in Table 2 [Tab. 2] and Figure 2 [Fig. 2], despite different EPT levels, pain intensity scores obtained by the female (1.9 (1.2–3.0) VAS units) did not differ (p>0.300) from those obtained by the male (2.0 (1.1–3.4) VAS units), or between female and male subjects evaluated by the female or male investigators (p>0.300). Higher (p>0.300) pain intensity scores were reported during the first (2.1 (1.1–3.2) VAS units) than during the second (1.8 (1.2–3.1) VAS units) series of stimulation.
Discussion
This is the first study to confirm an influence of investigator gender on pain perception in response to electrical pain stimulation, as far as we know. Our findings of higher EPT levels in females and males investigated by a female than by a male are in partial agreement with results obtained in males in the early 1990s by cold (with lower pain intensity) [7] and in the mid-2000s by mechanical pressure (with higher pain threshold) [4]. However, since those investigators were dressed to emphasize their gender roles, those results were interpreted to primarily reflect influence of traditional gender role expectations, as also proposed in a survey of epidemiological and laboratory data on sex differences in pain perception [29]. Nevertheless, another study from the mid-2000s and a recent study, both based on heat-induced pain, not emphasizing traditional investigator gender roles in line with our study, have also reported higher pain thresholds in males evaluated by a neutrally dressed female [5], [6], representing more realistic clinical patient-physician interaction.
Furthermore, males subjected to heat reported lower pain intensity levels when investigated by a female than by a male [6], but with no corresponding change in heart rate, possibly reflecting a primarily psychosocial influence on pain perception.
Intimate study settings, with a calm and quiet one-to-one environment, have been reported to facilitate non-verbal patient-physician interaction [10], and could hence be considered to accordingly promote communication between study participants and investigators. Female television spokespeople have recently been reported to communicate more extensively non-verbally [30], e.g. by more frequent smiling and eye contact [31], and a neurophysiological study [32] has reported stronger empathic abilities of females dealing with pain in others. Hence, the intimate study setting, potentially promoting non-verbal communication and empathic interaction, might have contributed to the main findings of the present study.
Our statistically non-differing EPT levels between female and male study participants are in accordance with diverging results reported in early studies based on electrical stimulation [33]. Reviews of later studies, also including other modalities of stimulation, support differences [24], [34], [35] as well as no differences [35] in pain perception between subject genders. No differences in pain perception were reported between female and male study participants in response to pain induced by cold [27], heat [9], [13], or venous cannulation [28]. In contrast, female subjects had lower threshold levels of pain induced by electricity [10], [13], [16], [36], mechanical pressure [11], [14], [18], [19], [37], heat [12], [14], [17], or cold [8], or reported higher intensity levels of pain induced by heat [21], [23] or cold [7], [22].
Factors underlying sex or gender differences in pain perception – physiological as well as psychosocial – are not yet fully understood [24], [34]. Higher nociceptive discrimination in females subjected to heat-induced pain [21] might indicate that gender differences in pain perception reflect physiological rather than psychosocial factors in agreement with a recent review [38] implying impact of humoral factors on central mediation of pain. Moreover, the perception of pressure-induced pain has been reported to be more influenced by sex than by gender [11], [37], and higher thermal-induced pain thresholds in males have been associated with higher activity of the parasympathetic nerve system [39]. However, cognitive and social factors have also been proposed to partly explain higher pain perception in females [25] and particularly reflect gender role expectations [26], [27], which is in agreement with higher pain thresholds found in subjects considering themselves more masculine according to a previous review [40]. Differences in pain perception between female and male subjects, not adjusted for investigator gender [11], [12], [13], [14], [17], [18], [19], [36], might actually, at least in part, also reflect a psychosocial impact of investigator gender [41].
Although we involved only one investigator of each gender to avoid interindividual variation, whereas up to four female and four male investigators have been involved in similarly designed but unpaired studies [6], [8], [37], this might be considered as a study limitation, despite similar external appearance, body size, generation and profession, and use of a predefined verbal script. The study investigators were not blinded to the main purpose of the study, in contrast to a similar previous study [7], which might also be a limitation. Parallel use of two identical and calibrated electrical devices (to enable blinding of the participants to the main study purpose) might also be considered as a limitation.
Advantages of this study are the blinding of participants to the main study purpose (to avoid some psychosocial impact on pain perception) and of both participants and investigators to on-line EPT levels. The use of a valid and reliable [42], [43] investigator-independent stimulation device designed for this specific purpose instead of investigator-dependent ones [4], [5], [6], [7] is considered to be another advantage. Combining EPT determination with individual VAS scoring – considered as the gold standard for pain assessment [44] – empowers our findings.
Carry-over effects were avoided by allowing sufficient time between the study sessions, and order effects by the randomized paired cross-over study design not used in previous similar studies [4], [6], [7], [9], [21], [22], [23], [45]. Furthermore, our main results are supported by statistical significance levels also taking multiple comparisons into consideration.
In conclusion, our main findings of higher EPT levels despite equal pain intensity scores in females and in males evaluated by a female investigator contribute to a better understanding of investigator gender impact on pain perception. Since these results may also have clinical relevance, future studies on investigator gender and pain perception in clinical settings are desirable, particularly considering the predominance of female staff in modern healthcare.
Notes
Informed consent
Informed consent has been obtained from all study participants.
Ethical approval
This research in humans complies with all the relevant national regulations and institutional policies, was performed in accordance with the tenets of the Helsinki Declaration, and has been approved by the regional Human Research Ethics Review Board (Approval No. 2015/779), Lund, Sweden.
Funding
The study was supported by research grants provided by Region Skåne, Kristianstad, and by research funds administered by Lund University Faculty of Medicine, Lund, Sweden.
Competing interests
The authors declare that they have no competing interests.
References
[1] Greenspan JD, Craft RM, LeResche L, Arendt-Nielsen L, Berkley KJ, Fillingim RB, Gold MS, Holdcroft A, Lautenbacher S, Mayer EA, Mogil JS, Murphy AZ, Traub RJ; Consensus Working Group of the Sex, Gender, and Pain SIG of the IASP. Studying sex and gender differences in pain and analgesia: a consensus report. Pain. 2007 Nov;132(Suppl 1):S26-S45. DOI: 10.1016/j.pain.2007.10.014[2] Daniali H, Flaten MA. A Qualitative Systematic Review of Effects of Provider Characteristics and Nonverbal Behavior on Pain, and Placebo and Nocebo Effects. Front Psychiatry. 2019 Apr;10:242. DOI: 10.3389/fpsyt.2019.00242
[3] Dubin AE, Patapoutian A. Nociceptors: the sensors of the pain pathway. J Clin Invest. 2010 Nov;120(11):3760-72. DOI: 10.1172/JCI42843
[4] Gijsbers K, Nicholson F. Experimental pain thresholds influenced by sex of experimenter. Percept Mot Skills. 2005 Dec;101(3):803-7. DOI: 10.2466/pms.101.3.803-807
[5] Sellgren Engskov A, Rubin AT, Åkeson J. Single and double pain responses to individually titrated ultra-short laser stimulation in humans. BMC Anesthesiol. 2019 Mar;19(1):29. DOI: 10.1186/s12871-019-0702-1
[6] Aslaksen PM, Myrbakk IN, Høifødt RS, Flaten MA. The effect of experimenter gender on autonomic and subjective responses to pain stimuli. Pain. 2007 Jun;129(3):260-8. DOI: 10.1016/j.pain.2006.10.011
[7] Levine FM, Lee De Simone L. The effects of experimenter gender on pain report in male and female subjects. Pain. 1991 Jan;44(1):69-72. DOI: 10.1016/0304-3959(91)90149-R
[8] Kállai I, Barke A, Voss U. The effects of experimenter characteristics on pain reports in women and men. Pain. 2004 Nov;112(1-2):142-7. DOI: 10.1016/j.pain.2004.08.008
[9] Essick G, Guest S, Martinez E, Chen C, McGlone F. Site-dependent and subject-related variations in perioral thermal sensitivity. Somatosens Mot Res. 2004 Sep-Dec;21(3-4):159-75. DOI: 10.1080/08990220400012414
[10] Hall JA, Irish JT, Roter DL, Ehrlich CM, Miller LH. Gender in medical encounters: an analysis of physician and patient communication in a primary care setting. Health Psychol. 1994 Sep;13(5):384-92. DOI: 10.1037//0278-6133.13.5.384
[11] Kröner-Herwig B, Gaßmann J, Tromsdorf M, Zahrend E. The effects of sex and gender role on responses to pressure pain. Psychosoc Med. 2012 Feb;9:Doc01. DOI: 10.3205/psm000079
[12] Kuhtz-Buschbeck JP, Andresen W, Göbel S, Gilster R, Stick C. Thermoreception and nociception of the skin: a classic paper of Bessou and Perl and analyses of thermal sensitivity during a student laboratory exercise. Adv Physiol Educ. 2010;34(2):25-34. DOI: 10.1152/advan.00002.2010
[13] Lautenbacher S, Rollman GB. Sex differences in responsiveness to painful and non-painful stimuli are dependent upon the stimulation method. Pain. 1993 Jun;53(3):255-64. DOI: 10.1016/0304-3959(93)90221-A
[14] Neziri AY, Scaramozzino P, Andersen OK, Dickenson AH, Arendt-Nielsen L, Curatolo M. Reference values of mechanical and thermal pain tests in a pain-free population. Eur J Pain. 2011 Apr;15(4):376-83. DOI: 10.1016/j.ejpain.2010.08.011
[15] Vigil JM, Rowell LN, Alcock J, Maestes R. Laboratory personnel gender and cold pressor apparatus affect subjective pain reports. Pain Res Manag. 2014 Jan-Feb;19(1):e13-8. DOI: 10.1155/2014/213950
[16] Lund I, Lundeberg T, Kowalski J, Svensson E. Gender differences in electrical pain threshold responses to transcutaneous electrical nerve stimulation (TENS). Neurosci Lett. 2005 Feb;375(2):75-80. DOI: 10.1016/j.neulet.2004.10.068
[17] Averbeck B, Seitz L, Kolb FP, Kutz DF. Sex differences in thermal detection and thermal pain threshold and the thermal grill illusion: a psychophysical study in young volunteers. Biol Sex Differ. 2017 Sep;8(1):29. DOI: 10.1186/s13293-017-0147-5
[18] Chesterton LS, Barlas P, Foster NE, Baxter DG, Wright CC. Gender differences in pressure pain threshold in healthy humans. Pain. 2003 Feb;101(3):259-66. DOI: 10.1016/S0304-3959(02)00330-5
[19] Garcia E, Godoy-Izquierdo D, Godoy JF, Perez M, Lopez-Chicheri I. Gender differences in pressure pain threshold in a repeated measures assessment. Psychol Health Med. 2007 Oct;12(5):567-79. DOI: 10.1080/13548500701203433
[20] Ferentzi E, Geiger M, Mai-Lippold SA, Köteles F, Montag C, Pollatos O. Interaction Between Sex and Cardiac Interoceptive Accuracy in Measures of Induced Pain. Front Psychol. 2021 Feb;11:577961. DOI: 10.3389/fpsyg.2020.577961
[21] Feine JS, Bushnell CM, Miron D, Duncan GH. Sex differences in the perception of noxious heat stimuli. Pain. 1991 Mar;44(3):255-62. DOI: 10.1016/0304-3959(91)90094-E
[22] Vigil JM, DiDomenico J, Strenth C, Coulombe P, Kruger E, Mueller AA, Guevara Beltran D, Adams I. Experimenter Effects on Pain Reporting in Women Vary across the Menstrual Cycle. Int J Endocrinol. 2015;2015:520719. DOI: 10.1155/2015/520719
[23] Fillingim RB, Edwards RR, Powell T. The relationship of sex and clinical pain to experimental pain responses. Pain. 1999 Dec;83(3):419-25. DOI: 10.1016/S0304-3959(99)00128-1
[24] Hanan G. Eltumi OAT. Effect of age, sex and gender on pain sensitivity: A narrative review. Open Pain J. 2017 Jul;10:44-55. DOI: 10.2174/1876386301710010044
[25] Racine M, Tousignant-Laflamme Y, Kloda LA, Dion D, Dupuis G, Choinière M. A systematic literature review of 10 years of research on sex/gender and pain perception – part 2: do biopsychosocial factors alter pain sensitivity differently in women and men? Pain. 2012 Mar;153(3):619-35. DOI: 10.1016/j.pain.2011.11.026
[26] Wandner LD, Scipio CD, Hirsh AT, Torres CA, Robinson ME. The perception of pain in others: how gender, race, and age influence pain expectations. J Pain. 2012 Mar;13(3):220-7. DOI: 10.1016/j.jpain.2011.10.014
[27] Robinson ME, Gagnon CM, Riley JL 3rd, Price DD. Altering gender role expectations: effects on pain tolerance, pain threshold, and pain ratings. J Pain. 2003 Jun;4(5):284-8. DOI: 10.1016/s1526-5900(03)00559-5
[28] Kivrak Y, Kose-Ozlece H, Ustundag MF, Asoglu M. Pain perception: predictive value of sex, depression, anxiety, somatosensory amplification, obesity, and age. Neuropsychiatr Dis Treat. 2016 Aug;12:1913-8. DOI: 10.2147/NDT.S106974
[29] Mogil JS. Sex differences in pain and pain inhibition: multiple explanations of a controversial phenomenon. Nat Rev Neurosci. 2012 Dec;13(12):859-66. DOI: 10.1038/nrn3360
[30] Iyanga-Mambo E. Gender-based verbal and nonverbal communication: A case study of spokespeople in British TV advertisement testimonials. South J Ling. 2017;41:95-118.
[31] Spangler L. Gender-specific nonverbal communication: Impact for speaker effectiveness. Hum Res Develop Quart. 1995;6(4):409-19. DOI: 1002/hrdq.3920060409
[32] Han S, Fan Y, Mao L. Gender difference in empathy for pain: an electrophysiological investigation. Brain Res. 2008 Feb;1196:85-93. DOI: 10.1016/j.brainres.2007.12.062
[33] Riley JL 3rd, Robinson ME, Wise EA, Myers CD, Fillingim RB. Sex differences in the perception of noxious experimental stimuli: a meta-analysis. Pain. 1998 Feb;74(2-3):181-7. DOI: 10.1016/s0304-3959(97)00199-1
[34] Bartley EJ, Fillingim RB. Sex differences in pain: a brief review of clinical and experimental findings. Br J Anaesth. 2013 Jul;111(1):52-8. DOI: 10.1093/bja/aet127
[35] Racine M, Tousignant-Laflamme Y, Kloda LA, Dion D, Dupuis G, Choinière M. A systematic literature review of 10 years of research on sex/gender and experimental pain perception – part 1: are there really differences between women and men? Pain. 2012 Mar;153(3):602-18. DOI: 10.1016/j.pain.2011.11.025
[36] Käll LB, Kowalski J, Stener-Victorin E. Assessing pain perception using the Painmatcher in patients with whiplash-associated disorders. J Rehabil Med. 2008 Mar;40(3):171-7. DOI: 10.2340/16501977-0163
[37] Otto MW, Dougher MJ. Sex differences and personality factors in responsivity to pain. Percept Mot Skills. 1985 Oct;61(2):383-90. DOI: 10.2466/pms.1985.61.2.383
[38] Sorge RE, Totsch SK. Sex Differences in Pain. J Neurosci Res. 2017 Jun;95(6):1271-81. DOI: 10.1002/jnr.23841
[39] Tracy LM, Koenig J, Georgiou-Karistianis N, Gibson SJ, Giummarra MJ. Heart rate variability is associated with thermal heat pain threshold in males, but not females. Int J Psychophysiol. 2018 Sep;131:37-43. DOI: 10.1016/j.ijpsycho.2018.02.017
[40] Alabas OA, Tashani OA, Tabasam G, Johnson MI. Gender role affects experimental pain responses: a systematic review with meta-analysis. Eur J Pain. 2012 Oct;16(9):1211-23. DOI: 10.1002/j.1532-2149.2012.00121.x
[41] Chapman CD, Benedict C, Schiöth HB. Experimenter gender and replicability in science. Sci Adv. 2018 Jan;4(1):e1701427. DOI: 10.1126/sciadv.1701427
[42] Lundeberg T, Lund I, Dahlin L, Borg E, Gustafsson C, Sandin L, Rosén A, Kowalski J, Eriksson SV. Reliability and responsiveness of three different pain assessments. J Rehabil Med. 2001 Nov;33(6):279-83. DOI: 10.1080/165019701753236473
[43] Stener-Victorin E, Kowalski J, Lundeberg T. A new highly reliable instrument for the assessment of pre- and postoperative gynecological pain. Anesth Anal. 2002 Jul;95(1):151-7. DOI: 10.1097/00000539-200207000-00027
[44] Myles PS, Urquhart N. The linearity of the visual analogue scale in patients with severe acute pain. Anaesth Intensive Care. 2005 Feb;33(1):54-8. DOI: 10.1177/0310057X0503300108
[45] Vigil JM, Rowell LN, Chouteau S, Chavez A, Jaramillo E, Neal M, Waid D. Sex differences in how social networks and relationship quality influence experimental pain sensitivity. PLoS One. 2013 Nov;8(11):e78663. DOI: 10.1371/journal.pone.0078663

