[Bewusstsein für und Einhaltung von Infektionskontrolle durch Studenten und Praktikanten der Zahnmedizin an der Riyadh Elm University]
Sultan Binalrimal 1Abdulmajed AlDrees 2
Mohammed AlWehaibi 2
Mohammed AlAsmary 3
Abdulaziz AlShammery 4
Essam AlHaidri 5
Lama AlQabbaa 6
1 Restorative Dentistry Department, Riyadh Elm University, Riyadh, Saudi Arabia
2 Riyadh, Saudi Arabia
3 Prosthodontics Department, King Salman Armed Forces Hospital – North Western Region, Tabuk, Saudi Arabia
4 Public Health Department, Riyadh Elm University, Riyadh, Saudi Arabia
5 Ministry of Health, Riyadh, Saudi Arabia
6 Riyadh Elm University, Riyadh, Saudi Arabia
Zusammenfassung
Zielsetzung: Zahnmedizinstudenten und Praktikanten sind während ihrer klinischen Ausbildung Infektionsrisiken ausgesetzt. Daher sollte die Einhaltung der Schutzmaßnahmen der Auszubildenden an der Riyadh Elm University, Saudi Arabien, analysiert werden.
Methode: Es wurden 400 Fragebögen mit 32 Items zur Einhaltung ausgewählter Präventionsmaßnahmen ausgegeben. Die Daten wurden mittels SPSS deskriptiv ausgewertet.
Ergebnisse: 309 Fragebögen waren auswertbar (Response Rate 77%). Die Implementierung der Präventionsmaßnahmen war mit Ausnahme der HBV-Schutzimpfung und des Tragens einer Schutzbrille gut bis sehr gut. Geimpft waren jedoch nur 76% der männlichen and 83% der weiblichen Personen. Augenschutz trugen sogar nur 30% der männlichen and 26% der weiblichen Personen.
Schlussfolgerung: Im Vergleich zu vorangegangen Analysen wurde ein gesteigertes Bewusstsein für Infektionskontrollpraktiken bei zahnmedizinischen Studenten und Praktikanten festgestellt. Es ist jedoch notwendig, dass alle Auszubildenden zur HBV-Schutzimpfung und zum Tragen von Schutzbrillen motiviert werden.
Schlüsselwörter
Kreuzinfektion, Infektionskontrolle, Zahnmedizinstudenten, Zahnmedizinische Praktikanten
Introduction
Dental health care workers (DHCW) are at a high risk of cross-infection through occupational exposure, such as needlestick and sharp instrument injuries (NSIs), mucocutaneous contamination, bites, conjuctivitis and mechanical trauma. The eyes are at particular risk from floating particles, which are considered serious hazards for DHCW, because they can transmit various microorganisms, e.g., cytomegalovirus, Mycobacterium tuberculosis, hepatitis B and hepatitis C viruses (HBV and HCV), Herpes simplex virus type 1, human immunodeficiency virus (HIV), streptococci, transmissible spongiform encephalopathies (including variant CJD), methicillin-resistant Staphylococcus aureus (MRSA), and severe acute respiratory syndrome (SARS) virus transmitted through direct and indirect contact [1], [2], [3], [4], [5], [6], [7], [8], [9], [10], [11], [12], [13], [14], [15], [16], [17].
The majority of infections are subclinical and almost 80% of all HBV infections are undiagnosed. Therefore, DHCW are at risk every day, because at normal working distances, there is no zone of safety for the risk of cross-infection. The danger is enhanced by the fact that some hazardous microorganisms remain in the air for up to 30 minutes after cavity excavation, and the fact that most human microbial pathogens have been isolated from oral secretions [7], [8], [18], [19], [20].
In 1946, Humphrey [21] described how three dental staff members developed different infections including syphilis, diphtheria and actinomycosis during the treatment of infected patients. The protection of health workers became imperative, especially with the rise of of the AIDS epidemic in the 1980s [22].
Routine infection control procedures and recommendations have been available since the 1970s, but were neglected and ignored even by highly educated groups. In 1996, the US Centers for Disease Control and Prevention (CDC) adopted the term “standard precautions” to generate broader understanding and awareness of prevention and transmission of infection. In 2003, the CDC published “Guidelines for Infection Control in Dental Health-Care Settings”, which included standard precautions to ensure safe working environments and prevent cross-infection among DHCW and their patients, and in 2016 the CDC published “Summary of Infection Prevention Practices in Dental Settings: Basic Expectations for Safe Care” [22], [23], [24], [25].
Despite the emphasis that was placed on making DHCW aware of the risk of cross-infection and the recommended practices to control infection transmission, the percentage of DHCW who adhered to those practices was below expectations [1], [2], [4], [9], [26], [27], [28], [29], [30], [31], [32], [33], [34], [35], [36], [37], [38].
Even at dental schools, dental students did not comply with infection control practices very well [13], [31], [34], [39], [40], [41], [42], [43], [44], [45], [46], [47], [48], [49], [50], [51].
Because dental students have increasing patient contact during their education and clinical years, they are at massive risk of cross-infection. Therefore, the aim of this study was to determine the level of compliance with infection control practices among dental students and interns at Riyadh Elm University, Riyadh, Saudi Arabia.
Materials and methods
The study was approved by the Review Board and Ethics Committee of Riyadh Elm University. A total of 400 questionnaires were distributed among clinical students and interns at Riyadh Elm University, Riyadh, Saudi Arabia. The questionnaire was designed to cover different aspects of infection control practices in dental clinics including:
- aseptic techniques,
- patient screening and evaluation,
- personal protection,
- instrument sterilization,
- immunization against hepatitis B virus,
- surface disinfection, and
- equipment asepsis.
An informed consent was included in the questionnaire design and required to be signed by every participant. The questionnaire comprised 32 items assessing infection control practices among undergraduate dental students and interns at Riyadh Elm University. Out of 400 questionnaires sent, 309 forms were filled out and returned. Forty-two of the respondents were interns (21 female and 21 male), while 267 forms were received from both male and female clinical students (96 4th-year students, 85 5th-year students, 86 6th-year students). The results obtained from respondents were tabulated and analyzed using the Statistical Package for the Social Sciences, version 24 (SPSS Inc. Chicago, IL USA).
Results
309 questionnaires were answered by clinical dental students and interns from Riyadh Elm University. The distribution of respondents from male and female 4th-, 5th-, and 6th-year students and interns is shown in Table 1 [Tab. 1].
Table 1: Distribution of respondents in the college to 4th-, 5th-, and 6th-year students and interns both male and female
The level of implementation of basic applied infection control measures was found to be good to excellent, except for HBV vaccine coverage and wearing protective eyewear. The results showed that only 76% of males and 83% of females had HBV vaccination, and only 30% of males and 26% of females always wore protective eyewear (Table 2 [Tab. 2] and Table 3 [Tab. 3]).
Table 2: Level of implementation of basic infection control measures at the university dental school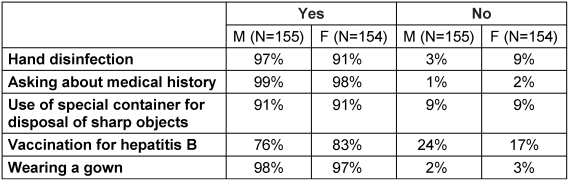
Table 3 : Level of implementation of basic infection control measures at the university dental school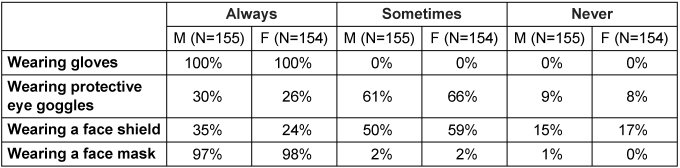
A majority of dental students and interns complied well with different infection control measures during the treatment of patients and between patients, but there is still a need to raise their awareness and improve their attitude regarding infection control practices. The infection control practices followed by dental students and interns during the treatment of patients and between patients are shown in Table 4 [Tab. 4].
Table 4: Infection control measures followed during treatment and between patients in the clinic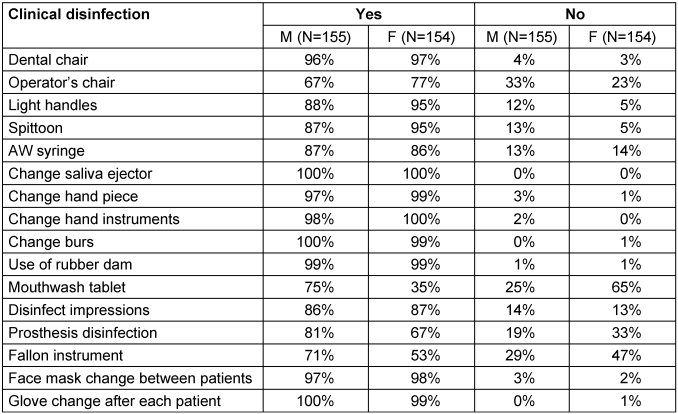
Discussion
Infection control is a dynamic and ever-changing discipline. Standard isolation precautions are designed to reduce the risk of acquiring occupational infections from both known and unknown sources in healthcare settings. Awareness of and compliance with these recommendations are crucial for the prevention of infections among healthcare workers (HCW), including dental healthcare professionals. The recrudescence of diseases such as HIV, tuberculosis, hepatitis B and C, and other maladies that were on the decline have made it essential that strict sterilization be maintained. The results of this study showed that the implementation of different infection control measures was good to excellent, except for hepatitis B vaccination and wearing eye protection.
Saudi Arabia was one of the HBV-endemic countries with an overall prevalence of 8.3%. The infection was mostly spread through horizontal transmission in early life. Over the years, there has been an enormous decrease in HBV incidence in Saudi Arabia, and the prevalence rate in 2009 was found to be 1.31% which places Saudi Arabia among the countries with the lowest prevalence rate of HBV worldwide [12], [13], [14], [15], [16], [17]. Unfortunately, previous studies reported that HCW in Saudi Arabia showed low compliance with hepatitis B vaccination, and it became mandatory to structure educational programs to raise the awareness and enhance health-care workers’ compliance with HBV vaccination [26], [37], [38]. It is noteworthy that HBV vaccination compliance was also below expectations among HCW in Brazil, Serbia, Libya, Ethiopia, China and India [10], [11], [25], [26], [27], [28], [35], [36], [42].
In previous studies investigating dental students’ and interns’ knowledge of, attitude toward and compliance with HBV vaccination among private and governmental dental schools in Saudi Arabia, their attitude was positive regarding infection control protocols, but they unfortunately lacked compliance with HBV vaccination; greater emphasis on the importance of immunization and vaccine coverage was needed. In our study population the compliance was greater than that of these other studies [33], [37], [45], [46], [47], [48], [49], [50] but still in need of improvement.
The results of this study demonstrate a need to further emphasize eye protection. The importance of protective eyewear was found to be in the interest of both dentist and patient due to the hazards associated with aerosols and floating debris. The use of eye protections with side shields, and regular monitoring of its structural integrity, reduces the risk of conjunctivitis, eye damage or even complete loss of vision [8].
The use of protective eyewear by dental students, interns and dentists in Saudi Arabia was found to be low in previous studies [33], [37], [45], [46], [47], [48], [49], [50]. In our study population the compliance was greater, but still in need of improvement.
In addition, the low compliance with eye protection was reported among DHCW and students in Lebanon, Morocco, India, and China [30], [35], [36], [40], [42].
It is the ethical obligation of every health care worker to safeguard themselves and their patients from cross-infection. Because the community expects zero risk of infection transmission from health care providers, a novel, more effective approach is needed to raise the awareness of the importance of vaccine coverage, protective eyewear, and adherence to infection control protocols.
Conclusion
Dental students tend to practice infection control measures they acquired during their clinical practice, and they are the future dental professionals who will provide oral healthcare to the population. Therefore, it is the responsibility of every academic institution to facilitate an appropriate preclinical immunization program, provide infection control training to protect students and patients from cross-infection, and educate the future healthcare professionals about safe work practices. The results of this study indicated increased awareness among concerned dental students and interns at Riyadh Elm University towards the implementation of effective infection control measures. Despite the increase awareness, more emphasis on the importance of compliance with HBV vaccination and the adherence to protective eyewear is needed.
Notes
Competing interests
The authors declare that they have no competing interests.
References
[1] Al-Zoughool M, Al-Shehri Z. Injury and infection in dental clinics: Risk factors and prevention. Toxicol Ind Health. 2018 Sep;34(9):609-619. DOI: 10.1177/0748233718769553[2] Shaghaghian S, Pardis S, Mansoori Z. Knowledge, attitude and practice of dentists towards prophylaxis after exposure to blood and body fluids. Int J Occup Environ Med. 2014 Jul;5(3):146-54.
[3] Tejera-Hernández CDL, Noyola D, Sánchez-Vargas L, Nava-Zárate N, Cruz-Mendoza EDL, Gómez-Hernández A, Aranda-Romo S. Analysis of risk factors associated to cytomegalovirus infection in dentistry students. J Oral Res. 2015;4(3):197-204. DOI: 10.17126/joralres.2015.039
[4] Dahiya P, Kamal R, Sharma V, Kaur S. “Hepatitis” – Prevention and management in dental practice. J Educ Health Promot. 2015;4:33.
[5] Mirza MB, Bhagat TV, Inderjit MG, Aljeaidi ZA. Middle East respiratory syndrome and precautions to be taken by dental surgeons. J Health Spec. 2016;4(2):105-9. DOI: 10.4103/1658-600X.179821
[6] Roberts MC, Soge OO, Horst JA, Ly KA, Milgrom P. Methicillin-resistant Staphylococcus aureus from dental school clinic surfaces and students. Am J Infect Control. 2011 Oct;39(8):628-32. DOI: 10.1016/j.ajic.2010.11.007
[7] Bhat N, Patel R, Reddy JJ, Singh S, Sharma A, Multani S. Knowledge and Awareness of Eye Flu among the Dentists and Dental Auxiliaries of Udaipur City, Rajasthan. Int J Prev Med. 2014 Jul;5(7):920-3.
[8] Ekmekcioglu H, Unur M. Eye-related trauma and infection in dentistry. J Istanb Univ Fac Dent. 2017;51(3):55-63. DOI: 10.17096/jiufd.60117
[9] Abeje G, Azage M. Hepatitis B vaccine knowledge and vaccination status among health care workers of Bahir Dar City Administration, Northwest Ethiopia: a cross sectional study. BMC Infect Dis. 2015 Jan;15:30. DOI: 10.1186/s12879-015-0756-8
[10] Peeran S, Peeran S, Mugrabi MA, Abdalla K, Murugan M, Alsaid F. Hepatitis B. Knowledge and attitude of graduating dentists from faculty of dentistry, Sebha University, Libya. Dent Med Res. 2017;5(1):3. DOI: 10.4103/2348-1471.198785
[11] Kisic-Tepavcevic D, Kanazir M, Gazibara T, Maric G, Makismovic N, Loncarevic G, Pekmezovic T. Predictors of hepatitis B vaccination status in healthcare workers in Belgrade, Serbia, December 2015. Euro Surveill. 2017 Apr;22(16). pii=30515. DOI: 10.2807/1560-7917.ES.2017.22.16.30515
[12] Arya SC, Ashraf SJ, Parande CM, el-Sayed M, Sahay R, Ageel AR, Tobeiqi MS. Hepatitis B virus in Gizan, Saudi Arabia. J Med Virol. 1985 Nov;17(3):267-74. DOI: 10.1002/jmv.1890170308
[13] Al-Hazmi AH. Knowledge, attitudes and practice of dentists concerning the occupational risks of hepatitis B virus in Al Jouf Province, Saudi Arabia. Niger J Clin Pract. 2015 Mar-Apr;18(2):276-81. DOI: 10.4103/1119-3077.151067
[14] Al-Faleh FZ, Ayoola EA, Arif M, Ramia S, al-Rashed R, al-Jeffry M, al-Mofarreh M, al-Karawi M, al-Shabrawy M. Seroepidemiology of hepatitis B virus infection in Saudi Arabian children: a baseline survey for mass vaccination against hepatitis B. J Infect. 1992 Mar;24(2):197-206. DOI: 10.1016/0163-4453(92)93006-C
[15] AlFaleh F, Alshehri S, Alansari S, Aljeffri M, Almazrou Y, Shaffi A, Abdo AA. Long-term protection of hepatitis B vaccine 18 years after vaccination. J Infect. 2008 Nov;57(5):404-9. DOI: 10.1016/j.jinf.2008.08.008
[16] Alswaidi FM, O'Brien SJ. Is there a need to include HIV, HBV and HCV viruses in the Saudi premarital screening program on the basis of their prevalence and transmission risk factors? J Epidemiol Community Health. 2010 Nov;64(11):989-97. DOI: 10.1136/jech.2009.093302
[17] Abdo AA, Sanai FM, Al-Faleh FZ. Epidemiology of viral hepatitis in Saudi Arabia: are we off the hook? Saudi J Gastroenterol. 2012 Nov-Dec;18(6):349-57. DOI: 10.4103/1319-3767.103425
[18] Tzukert A, Sandler SG. Dental care and spread of hepatitis B virus infection. J Clin Microbiol. 1978 Sep;8(3):302-5.
[19] Larato DC, Ruskin PF, Martin A, Delanko R. Effect of a dental air turbine drill on the bacterial counts in air. J Prosthet Dent. 1966;16(4):758-65. DOI: 10.1016/0022-3913(66)90157-0
[20] Narasimhan M, Hazarey VK, Varadarajan S. Prevalence of Hepatitis B surface antigen in dental personnel. J Oral Maxillofac Pathol. 2015 Jan-Apr;19(1):34-6. DOI: 10.4103/0973-029X.157198
[21] Humphreys HF. Notes on three cases of specific infections of the hand in dental surgeons. Br Dent J. 1946 Jun;80:367. DOI: 10.1016/0030-4220(48)90291-6
[22] Assiri KI, Naheeda, Kaleem SM, Ibrahim M, Alam T, Asif SM. Knowledge, attitude, and practice of infection control among dental students in King Khalid University, Abha. J Int Oral Health. 2018;10(2):83. DOI: 10.4103/jioh.jioh_6_18
[23] Gerbert B. AIDS and infection control in dental practice: dentists’ attitudes, knowledge, and behavior. J Am Dent Assoc. 1987 Mar;114(3):311-4. DOI: 10.14219/jada.archive.1987.0078
[24] Kohn WG, Collins AS, Cleveland JL, Harte JA, Eklund KJ, Malvitz DM; Centers for Disease Control and Prevention (CDC). Guidelines for infection control in dental health-care settings--2003. MMWR Recomm Rep. 2003 Dec 19;52(RR-17):1-61.
[25] Centers for Disease Control and Prevention. Summary of Infection Prevention Practices in Dental Settings: Basic Expectations for Safe Care. Atlanta, GA: Centers for Disease Control and Prevention, US Dept of Health and Human Services; 2016 Oct.
[26] Hegazy AA, Albar HM, Albar NH. Hepatitis B Vaccination Coverage and Knowledge among Healthcare Workers at a Tertiary Hospital in Jeddah, Saudi Arabia. J Adv Med Pharm Sci. 2016 Oct;11(1):1-9. DOI: 10.9734/JAMPS/2016/30082
[27] Abebaw TA, Aderaw Z, Gebremichael B. Hepatitis B virus vaccination status and associated factors among health care workers in Shashemene Zonal Town, Shashemene, Ethiopia: a cross sectional study. BMC Res Notes. 2017 Jul;10(1):260. DOI: 10.1186/s13104-017-2582-0
[28] Resende VL, Abreu MH, Paiva SM, Teixeira R, Pordeus IA. Concerns regarding hepatitis B vaccination and post-vaccination test among Brazilian dentists. Virol J. 2010 Jul;7:154. DOI: 10.1186/1743-422X-7-154
[29] Gupta S, Rani S, Garg S. Infection control knowledge and practice: A cross-sectional survey on dental laboratories in dental institutes of North India. J Indian Prosthodont Soc. 2017 Oct-Dec;17(4):348-354. DOI: 10.4103/jips.jips_5_17
[30] Dagher J, Sfeir C, Abdallah A, Majzoub Z. Infection Control Measures in Private Dental Clinics in Lebanon. Int J Dent. 2017;2017:5057248. DOI: 10.1155/2017/5057248
[31] Sammy KC, Benjamin SN. Infection Control Mechanisms Employed by Dental Laboratories to Prevent Infection of their Dental Technicians/Technologists. J Oral Health Craniofac Sci. 2016;1:001-011. DOI: 10.29328/journal.johcs.1001001
[32] Althomairy SA, Baseer MA, Assery M, Alsaffan AD. Knowledge and Attitude of Dental Health Professionals about Middle East Respiratory Syndrome in Saudi Arabia. J Int Soc Prev Community Dent. 2018 Mar-Apr;8(2):137-144. DOI: 10.4103/jispcd.JISPCD_9_18
[33] La Torre G, Scalingi S, Garruto V, Siclari M, Chiarini M, Mannocci A. Knowledge, Attitude and Behaviours towards Recommended Vaccinations among Healthcare Workers. Healthcare (Basel). 2017 Mar;5(1):. DOI: 10.3390/healthcare5010013
[34] Yoo YJ, Kwak EJ, Jeong KM, Baek SH, Baek YS. Knowledge, attitudes and practices regarding methicillin-resistant Staphylococcus aureus (MRSA) infection control and nasal MRSA carriage rate among dental health-care professionals. Int Dent J. 2018 Oct;68(5):359-366. DOI: 10.1111/idj.12388
[35] Wu L, Yin YL, Song JL, Chen Y, Wu YF, Zhao L. Knowledge, attitudes and practices surrounding occupational blood-borne pathogen exposure amongst students in two Chinese dental schools. Eur J Dent Educ. 2016 Nov;20(4):206-212. DOI: 10.1111/eje.12162
[36] Bommireddy VS, Pachava S, Sanikommu S, Vinnakota NR, Talluri D, Ghanta BK. Infection control measures among dental practitioners in a Southern state of India: A cross-sectional study. J Indian Assoc Public Health Dent. 2016;14(3):302-7. DOI: 10.4103/2319-5932.187178
[37] Alqahtani JM, Abu-Eshy SA, Mahfouz AA, El-Mekki AA, Asaad AM. Seroprevalence of hepatitis B and C virus infections among health students and health care workers in the Najran region, southwestern Saudi Arabia: the need for national guidelines for health students. BMC Public Health. 2014 Jun;14:577. DOI: 10.1186/1471-2458-14-577
[38] Panhotra BR, Saxena AK, Al-Hamrani HA, Al-Mulhim A. Compliance to hepatitis B vaccination and subsequent development of seroprotection among health care workers of a tertiary care center of Saudi Arabia. Am J Infect Control. 2005 Apr;33(3):144-50. DOI: 10.1016/j.ajic.2005.01.002
[39] Pinelli C, do Nascimento Neri S, de Castro Monteiro Loffredo L. Dental students’ reports of occupational exposures to potentially infectious biological material in a Brazilian School of Dentistry. Cad Saude Colet. 2016;24(2):162-9. DOI: 10.1590/1414-462X201600020238
[40] Hbibi A, Kasouati J, Charof R, Chaouir S, El Harti K. Evaluation of the Knowledge and Attitudes of Dental Students toward Occupational Blood Exposure Accidents at the End of the Dental Training Program. J Int Soc Prev Community Dent. 2018 Jan-Feb;8(1):77-86.
[41] Shaghaghian S, Golkari A, Pardis S, Rezayi A. Occupational Exposure of Shiraz Dental Students to Patients’ Blood and Body Fluid. J Dent (Shiraz). 2015 Sep;16(3):206-13.
[42] Singh A, Purohit BM, Bhambal A, Saxena S, Singh A, Gupta A. Knowledge, attitudes, and practice regarding infection control measures among dental students in Central India. J Dent Educ. 2011 Mar;75(3):421-7.
[43] Alshiddi IF. Attitude and awareness of dental students and interns toward infection control measures in prosthodontic clinics. Dent Oral Craniofac Res. 2015;1(4):116-20. DOI: 10.15761/DOCR.1000128
[44] Halboub ES, Al-Maweri SA, Al-Jamaei AA, Tarakji B, Al-Soneidar WA. Knowledge, Attitudes, and Practice of Infection Control among Dental Students at Sana’a University, Yemen. J Int Oral Health. 2015 May;7(5):15-9.
[45] Al-Maweri SA, Tarakji B, Shugaa-Addin B, Al-Shamiri HM, Alaizari NA, AlMasri O. Infection control: Knowledge and compliance among Saudi undergraduate dental students. GMS Hyg Infect Control. 2015;10:Doc10. DOI: 10.3205/dgkh000253
[46] Al-Essa NA, Almutairi MA. To what extent do dental students comply with infection control practices? Saudi J Dent Res. 2017;8(1-2):67-72. DOI: 10.1016/j.sjdr.2016.10.003
[47] Al-Shamiri HM, AlShalawi FE, AlJumah TM, AlHarthi MM, AlAli EM, AlHarthi HM. Knowledge, Attitude and Practice of Hepatitis B Virus Infection among Dental Students and Interns in Saudi Arabia. J Clin Exp Dent. 2018 Jan;10(1):e54-e60. DOI: 10.4317/jced.54418
[48] Ahmad IA, Rehan EA, Pani SC. Compliance of Saudi dental students with infection control guidelines. Int Dent J. 2013 Aug;63(4):196-201. DOI: 10.1111/idj.12030
[49] Alanazi AO, Alrawili YK, Alanazi YM, Shah FA. Knowledge and Attitudes towards Infection Control Protocols among the Students of Al-Jouf University in Saudi Arabia. Egypt J Hosp Med. 2018 Apr;71(6):3328-31.
[50] Adenlewo OJ, Adeosun PO, Fatusi OA. Medical and dental students’ attitude and practice of prevention strategies against hepatitis B virus infection in a Nigerian university. Pan Afr Med J. 2017;28:33. DOI: 10.11604/pamj.2017.28.33.11662
[51] Mandourh MS, Alhomaidhi NR, Fatani NH, Alsharif AS, Ujaimi GK, Khan GM, Afifi IK. Awareness and implementation of infection control measures in private dental clinics, Holy Makkah, Saudi Arabia. Int J Infect Control. 2017;13(1).

