Uterine peaking – sonographic sign of vesico-uterine adhesion
Mohammad Sami Walid 1Richard L. Heaton 1
1 Heart of Georgia Women's Center, Warner Robins, GA, USA
Abstract
Objective: In this paper we present our observation of a specific sign on transvaginal ultrasound that may help basic minimal invasive surgeons diagnose vesico-uterine adhesions preoperatively.
Methods: The ultrasound images of the latest eleven patients who were preoperatively diagnosed with vesico-uterine adhesions using transvaginal ultrasound were compared with their intraoperative findings.
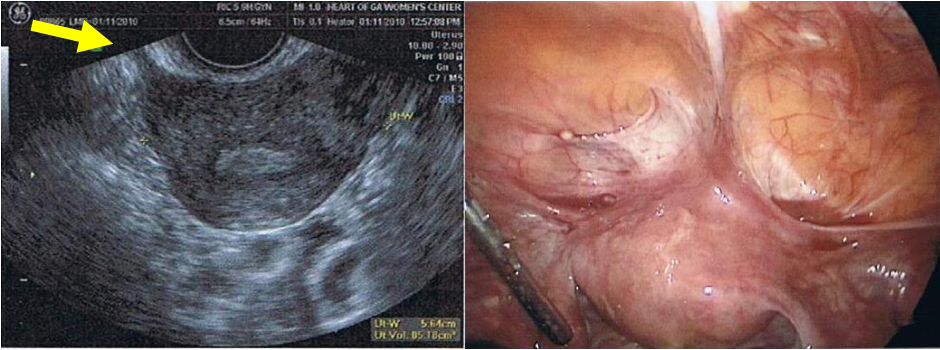
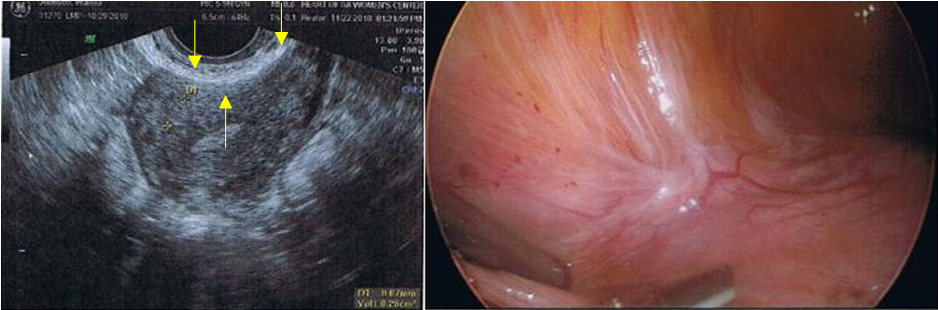
Results: Ultrasonography showed a spectrum of changes from obliterated anterior cul-de-sac to dense fibrosis between the lower uterine segment and cervix with the bladder. Horn- or beak-shaped streaks of tissue with the same density of uterine myometrium is a sign of fundal attachment of vesico-uterine adhesions or of complete anterior cul-de-sac obliteration with adhesions going between the uterus and the anterior abdominal wall. Fine papillary peaking is seen in cases of dense lower uterine segment and cervical fibrosis without fundal involvement. These signs combined with limited mobility of the cervix and bladder base correlated with the presence of dense vesico-uterine adhesions.
Conclusion: The described sonographic signs, two static and the other dynamic, may help basic minimal invasive gynecological surgeons who do not have advanced laparoscopic skills and do not feel comfortable dealing with an obliterated anterior cul-de-sac or dense vesico-uterine space fibrosis predict the presence of dense vesico-uterine adhesions allowing them to choose another route that they may be more comfortable with such as vaginal or abdominal hysterectomy or request assistance from a more experienced colleague.
Keywords
uterine peaking, ultrasound, vesico-uterine adhesion
Introduction
Caesarean section (C-section) is the most common surgical procedure in women, estimated at around 30.5% of deliveries in the United States [1]. Internal adhesions and scar tissue are a very common side effect of this procedure. Adhesions begin forming almost immediately after surgery and for many women adhesions are painless and remain silent; however for others they may cause chronic pelvic pain, dyspareunia, or even bowel obstruction [2].
It is common belief among minimal invasive gynecological surgeons that a history of C-section is a strong contraindication to laparocopic hysterectomy due to the high risk of bladder injury during vesico-uterine dissection. Indeed, in some cases the anterior cul-de-sac appears completely obliterated by dense adhesions of the vesico-uterine reflection making laparoscopic dissection extremely challenging [3]. From our experience we describe a specific echographic sign that may help basic minimal invasive surgeons diagnose vesico-uterine adhesions preoperatively.
Materials and methods
The ultrasound images of the latest eleven patients who were preoperatively diagnosed with vesico-uterine adhesions using transvaginal ultrasound were compared with their intraoperative findings. All patients underwent laparoscopic procedures for gynecological indications including ten patients that had total laparoscopic hysterectomy. All patients were multiparous women with a history of C-section. Six patients (54.5%) had more than one C-section. Only one patient had endometriotic implants in the vesico-uterine adhesions. Seven patients (63.6%) had cystoscopic signs of interstitial cystitis (Table 1 [Tab. 1]).
Results
The ultrasound images showed evidence suggesting changes ranging from obliterated anterior cul-de-sac to simple dense vesico-uterine fibrosis between the lower uterine segment, cervix and bladder. Peaks of tissue with the same density of the uterus were evident between the uterus and the anterior abdominal wall or bladder reflection with peaking that is horn-shaped of the uterine fundus due to pulling by gravity in the supine position and scar contracture over time (indeed long horns of uterine tissue up to several inches are found in extreme cases at surgery). Fine papillary peaking was present in other patients with lower uterine segment and cervical vesico-uterine fibrosis. These signs combined with limited mobility of the cervix and bladder base when the cervix is pushed with the ultrasound transducer correlated completely (r=1, P=0) with the presence of dense vesico-uterine adhesions in the anterior cul-de-sac. We noticed two major forms of uterine peaking: wide, horn-shaped that implies abdominal wall attachment or contracture of anterior cul-de-sac scarring that involved the uterine fundus (any area above the lower uterine segment) resulting in either partial or complete obliteration of the anterior cul-de-sac (Figure 1 [Fig. 1]) and fine, papillary-shaped usually noted between the bladder base and lower uterine segment and cervix (Figure 2 [Fig. 2]) implying dense vesico-uterine adhesions and fixation of the normally areolar layer, the elastic mobile layer between the lower uterine segment, cervix and the bladder base. This is seen on ultrasound as multiple small papillary streaks of uterine density between this region and the bladder base.
Commentary
The described sonographic signs, two static and the other dynamic, may help basic minimal invasive gynecological surgeons who do not have advanced laparoscopic skills and do not feel comfortable dealing with an obliterated anterior cul-de-sac predict the presence of dense vesico-uterine adhesions and offer routes of surgery with which they are more comfortable or scrub with a more experienced colleague in order to advance their skill level. Patients with dense vesico-uterine adhesions are often women with multiple C-sections in their past and often suffer from deep penetration dyspareunia due to limited mobility of the cervix and bladder base [2]. This is a very common problem and can be very disruptive to marital relationship. These patients are given recommendations to use positional-avoidance techniques during intercourse, mainly female-dominant controlled positions or from behind on their side. Men usually cannot achieve deep penetration in the last position.
If conservative treatment does not work and the patient wants to preserve fertility she can have laparoscopic revision where the vesico-uterine adhesions are opened with the active edge of the harmonic scalpel turned in toward the uterus beginning from the left paravesical space above the uterine vessels to the right paravesical space taking little pieces of scar tissue at a time and stripping the entire scar tissue right off [3]. In women who have completed their reproductive function hysterectomy can be offered. The choice of procedure, abdominal, vaginal or laparoscopic, will however depend on the experience of the surgeon dealing with such delicate cases.
Notes
Competing interests
The authors certify that no actual or potential conflict of interest exists in relation to this article.
References
[1] Zhang J, Troendle J, Reddy UM, Laughon SK, Branch DW, Burkman R, Landy HJ, Hibbard JU, Haberman S, Ramirez MM, Bailit JL, Hoffman MK, Gregory KD, Gonzalez-Quintero VH, Kominiarek M, Learman LA, Hatjis CG, van Veldhuisen P; Consortium on Safe Labor. Contemporary cesarean delivery practice in the United States. Am J Obstet Gynecol. 2010;203(4):326.e1-326.e10. DOI: 10.1016/j.ajog.2010.06.058[2] Walid MS, Heaton RL. Dyspareunia: a complex problem requiring a selective approach. Sex Health. 2009;6(3):250-3. DOI: 10.1071/SH09033
[3] Walid MS, Heaton RL. Total laparoscopic hysterectomy with obliterated anterior cul-de-sac. GMS Ger Med Sci. 2010;8:Doc03. DOI: 10.3205/000092

