Case report of a cervical lipoleiomyoma with an incidentally discovered ovarian granulosa cell tumor – imaging and minimal-invasive surgical procedure
M. Sami Walid 1Richard L. Heaton 2
1 Medical Center of Central Georgia, Macon, GA, USA
2 Heart of Georgia Women's Center, Warner Robins, GA, USA
Abstract
Uterine lipoleiomyomas are rare benign tumors that mostly affect the uterine corpus. We are reporting the imaging and operative procedure of a very rare case of a large lipoleiomyoma of the uterine cervix combined with an occult adult ovarian granulosa cell tumor. The patient was treated with minimal invasive surgery.
Keywords
lipomeiomyoma, granulosa cell tumor, total laparoscopic hysterectomy
Case presentation
Uterine lipoleiomyoma is a rare benign tumor with an estimated incidence of 0.03% to 0.2% [1]. A 48 year-old, gravida 1 para 1, had a slowly-growing cervical mass. On ultrasound, the mass was around 5 cm in diameter and had fibroid tissue consistency with components of fat consistency (Figure 1 [Fig. 1]). On computed tomography (CT), the tumor appeared encapsulated and measured 6.2×5.2 cm with some areas of what looked like necrosis suggestive of a degenerating fibroid. No adenopathy was detected. The uterus was hypertrophic, sounding to 10 cm, and curettage showed no malignancy. After consultation with the patient, we decided to proceed with total laparoscopic hysterectomy and bilateral salpingo-oophorectomy. Operative findings included a large cervical fibroid that appeared somewhat fleshy and soft in texture (Figure 2 [Fig. 2]). First, the adhesions of the sigmoid colon to the left pelvic sidewall were taken down. The infundibulopelvic ligaments, after visualizing the ureters to be separate from them, were bilaterally coagulated and transected. The broad ligament anterior peritoneum was undermined and transected from round ligament to round ligament. The broad ligament posterior peritoneum was undermined and transected to the level of the uterosacral ligament on each side allowing the ureters to retract laterally away from the uterus, increasing the safety of the procedure. With some trouble, dissection was done to free the bladder from the cervical tumor. The vessels on the left side were then coagulated with bipolar cautery and transected with Harmonic scalpel. The cardinal ligament was taken down with Harmonic scalpel dissection. On the right side, again with difficulty the uterine vessels were skeletonized then coagulated and transected the same way as before. The cardinal ligament on this side was transected the same way. A sponge stick was placed in the anterior vagina and transverse incision was made over it and around the vagina separating it from the cervix. With the help of a tenaculum, the uterus with the cervical mass and adnexa were all removed and passed off. The operation was then continued as usual with uterosacral-cardinal-ligament suspension. Cystoscopy showed indogocarmine coming from both ureteral orifices, excluding ureteral injury. The operation was completed in 68 minutes and blood loss was approximately 150 cc. On opening of the resected tumor, no necrotic areas were noted. Pathological report showed a 258 gram uterus with a lipoleiomyoma that originated in the parametrial soft tissue along the endocervical canal near the lower uterine segment. The maximum dimension of the tumor was 5.5 cm. Incidentally, a 2.1 cm adult granulosa cell tumor was found within the parenchyma of the right ovary.
Figure 1: Ultrasound image of the cervical mass showing an echogenic mass with hypogenic components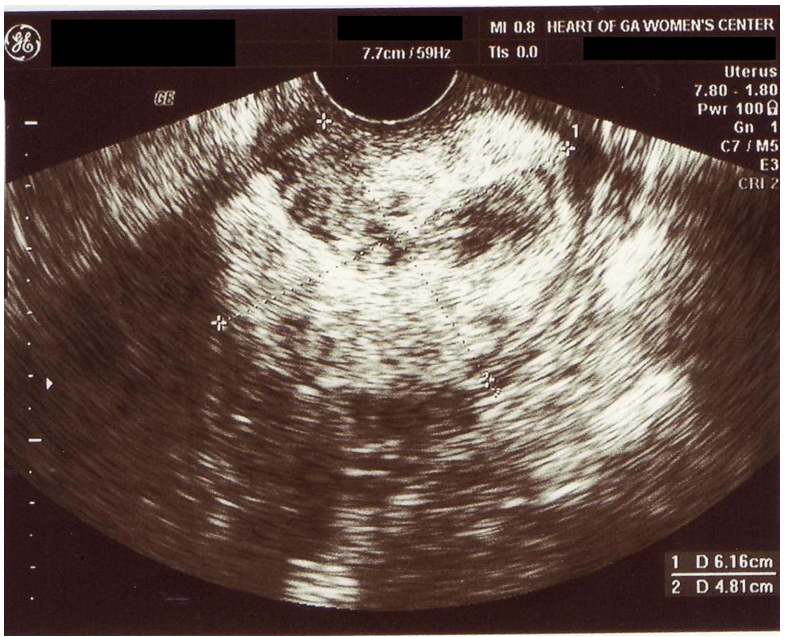
Figure 2: Laparoscopic view of the large cervical mass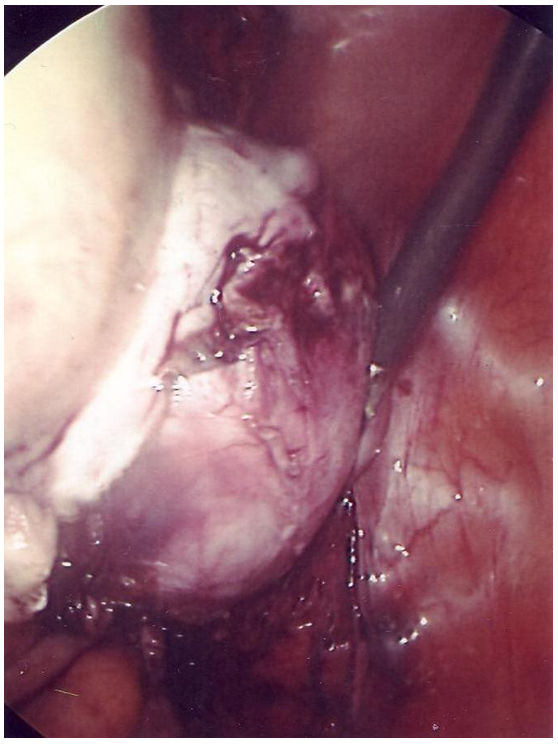
So, on ultrasound, a lipoleiomyoma can closely resemble a well-differentiated liposarcoma requiring more definitive imaging (CT or MRI), biopsy, or both to confirm its benign nature [2], [3], [4]. These tumors mostly affect the uterine corpus and less commonly the uterine cervix [4]. A similar case was reported by Avritscher et al. 2001 who described a woman of the same age with a 5-cm well-circumscribed complex mass that arose from the lower uterine segment and was markedly echogenic on sonography [5]. The route of treatment of that mass was not mentioned. Our case describes a combination of cervical lipomeiomyoma and ovarian adult granulosa cell tumor which has not been reported before. Moreover, our case demonstrates the feasibility of total laparoscopic extirpation of a uterus with a large cervical lipomeiomyoma attached to it if the surgeon has the experience and the will to do it.
Notes
Conflicts of interest
None declared.
References
[1] Prieto A, Crespo C, Pardo A, Docal I, Calzada J, Alonso P. Uterine lipoleiomyomas: US and CT findings. Abdom Imaging. 2000;25(6):655 -657. DOI: 10.1007/s002610000052[2] Tsushima Y, Kita T, Yamamoto K. Uterine lipoleiomyoma: MRI, CT and ultrasonographic findings. Br J Radiol. 1997;70(838):1068-70.
[3] Su WH, Wang PH, Chang SP, Su MC. Preoperational diagnosis of a uterine lipoleiomyoma using ultrasound and computed tomography images: a case report. Eur J Gynaecol Oncol. 2001;22(6):439-40.
[4] Wang X, Kumar D, Seidman JD. Uterine lipoleiomyomas: a clinicopathologic study of 50 cases. Int J Gynecol Pathol. 2006;25(3):239-42. DOI: 10.1097/01.pgp.0000192273.66931.29
[5] Avritscher R, Iyer RB, Ro J, Whitman G. Lipoleiomyoma of the uterus. AJR Am J Roentgenol. 2001;177(4):856.

