Foot-operated door opener to eliminate the door handle as a source of contamination
Stefan Preiss 1Axel Kramer 2
1 SASS-Systeme, Hannover, Germany
2 Institute of Hygiene and Environmental Medicine, University Medicine, Greifswald, Germany
Abstract
Aim: As door handles represent a transmission route for viruses and micro-organisms, a door opening and closing mechanism should be developed without manual operation.
Method: To solve the problem, a device for opening the door with the help of a foot pedal was built into the door leaf.
Results: The design enables mechanical opening of the door with a foot pedal without manual operation. Subsequently, the door closes with the help of a mechanical locking mechanism.
Discussion: The foot-operated door opener constitutes an additional option to the door handle. Together with the equipment of a soft closing mechanism, it is possible to prevent noise emanating from the door latch impinging on the door frame. Using this construction, the door handle as a transmission vector is eliminated. In addition, the transport of goods held with two hands simultaneously is facilitated.
Conclusion: With a foot-operated door opener instead of the traditional manual door handle, it is possible to open doors with a foot pedal. This prevents contamination of door handles with pathogens.
Keywords
door handle, risk of contamination, mechanical foot-operated door opener
Introduction
The increase in bacterial antibiotic resistance is a serious problem, increasing both in severity and importance [1]. Therefore, it is necessary to find means of limiting or even preventing the transmission of pathogens within medical facilities.
Surfaces in patients’ surroundings, including the door knob or handle, are a relevant transmission route for viruses and microorganisms [2], [3], [4], [5]. Hospital staff, visitors, cleaning services and others are a potential source of contamination for door handles. In particular, the nursing staff – with a hand-disinfection rate of under 50% [6], [7] – can spread pathogens, as can other employees, 4.6% of whom have been found to be colonized with MRSA [8]. Furthermore, pathogens can be acquired directly by the patient.
One alternative to avoid this route of transmission is to equip doors with a foot-operated door opener rather than with a door handle.
Methods
A device for opening the door with the foot was fitted flush into the door leaf. A pedal (Figure 1 [Fig. 1]) is integrated into the device, which is built into the bottom of the door leaf. To open the door, this pedal is pulled out with the foot from the inside of the device, while the foot constantly remains on the surface of the pedal. After completely pulling the pedal out, the door can be pushed open or pulled open while keeping light pressure on the pedal with the foot. The surface design of the pedal provides the necessary grip of the shoe on the pedal during the movement to be executed. Subsequently, the door will briefly remain in the open position before the door closer starts to pull the door back into its frame.
Figure 1: Door opener with optional hand or foot operation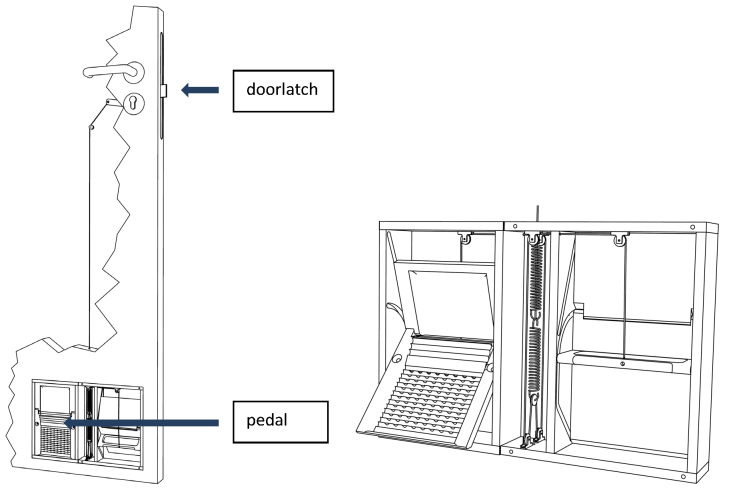
Results
Using the foot pedal alone, this device makes it possible to open the door without manual operation. After opening of the door, there is ample time to pass through the open door. The foot-operated door opener is optionally equipped with a soft-closing mechanism. As a result, while opening the door with the foot door opener, the door latch (Figure 1 [Fig. 1]) will be kept inside the door lock by a mechanism integrated into the foot door opener. Only after complete closing of the door (i.e., the door is back in its frame) is the door latch released by the mechanism: the door latch slowly and quietly returns to its normal position in the counterpart within the door frame.
Discussion
The foot-operated door opener constitutes an additional option to the door handle. The function of the door handle and the door lock itself is not affected. In both cases, opening with the door handle or foot-operated door opener, the door latch is triggered, which means a change in the mechanics of the normal door handle with its lock is not necessary. Only if the door lock itself is locked is it impossible to open the door with either the handle or the foot door opener. Equipped with the soft closing mechanism, the noise generated by the door latch hitting the door frame is completely prevented, and the noise generated by the door latch quickly snapping back into its counterpart in the door frame is almost imperceptible.
The foot door opener makes the door handle superfluous in most cases. This eliminates the risk of contamination by pathogens potentially adherent on the door handle. In addition, the transport of items that must be carried with both hands, e.g., trays, is facilitated.
Another means of opening doors without using the hands is provided by door handles designed to be operated with the forearm. However, this type of handle can still be operated by hand and is thus in danger of becoming contaminated. Nevertheless, when used correctly, the forearm-operated door opener reduces the risk of cross-infection [9].
Where door handles are coated with oligodynamic effective metals such as silver and copper in nanocrystalline form, the antimicrobial action takes effect only many hours later, and a false sense of security is produced. Based on unproven efficacy within a relevant exposure time, inactivation through protein loading [10], and the absence of evaluations on possible toxic risks, coating door handles with such compounds is not a reasonable alternative to the foot-operated door opener [11].
If used correctly, the mechanical foot-operated door opener can completely avoid the transfer of pathogens. Additional advantages include:
- no electrical energy is necessary for operation
- no follow-up costs arise, e.g., from consumables
- the functionality of the existing door lock is not compromised,and
- nothing protrudes from the plane of the door leaf.
Conclusion
With the foot-operated door opener described here instead of the traditional manually operated door handle, it is possible to open doors with a foot pedal. Contamination of door handles with pathogens is thus avoided.
Notes
Competing interests
Stefan Preiss is responsible for sales/production at SASS-Systeme GmbH
Axel Kramer declares that he has no competing interests.
References
[1] European Centre for Disease Prevention and Control. Antimicrobial resistance surveillance in Europe 2009. Annual Report of the European Antimicrobial Resistance Surveillance Network (EARS-Net). Stockholm: ECDC; 2010. Available from: http://ecdc.europa.eu/en/publications/Publications/1011_SUR_annual_EARS_Net_2009.pdf[2] Oie S, Hosokawa I, Kamiya A. Contamination of room door handles by methicillin-sensitive/methicillin-resistant Staphylococcus aureus. J Hosp Infect. 2002;51(2):140-3. DOI: 10.1053/jhin.2002.1221
[3] Oie S, Suenaga S, Sawa A, Kamiya A. Association between isolation sites of methicillin-resistant Staphylococcus aureus (MRSA) in patients with MRSA-positive body sites and MRSA contamination in their surrounding environmental surfaces. Jpn J Infect Dis. 2007;60(6):367-9.
[4] Barker J, Vipond IB, Bloomfield SF. Effects of cleaning and disinfection in reducing the spread of Norovirus contamination via environmental surfaces. J Hosp Infect. 2004;58(1):42-9. DOI: 10.1016/j.jhin.2004.04.021
[5] Dancer SJ. Importance of the environment in meticillin-resistant Staphylococcus aureus acquisition: the case for hospital cleaning. Lancet Infect Dis. 2008;8(2):101-13. DOI: 10.1016/S1473-3099(07)70241-4
[6] Pittet D. Improving compliance with hand hygiene in hospitals. Infect Control Hosp Epidemiol. 2000;21(6):381-6. DOI: 10.1086/501777
[7] Pittet D, Allegranzi B, Boyce J; World Health Organization World Alliance for Patient Safety First Global Patient Safety Challenge Core Group of Experts. The World Health Organization Guidelines on Hand Hygiene in Health Care and their consensus recommendations. Infect Control Hosp Epidemiol. 2009;30(7):611-22. DOI: 10.1086/600379
[8] Albrich WC, Harbarth S. Health-care workers: source, vector, or victim of MRSA? Lancet Infect Dis. 2008;8(5):289-301. DOI: 10.1016/S1473-3099(08)70097-5
[9] Seguier, Welker, Bourreau et al. Is it possible to reduce the risk of the colonisation of hands, thanks to the use of ULNA door-handles? SFHH Congrès 7.-8.6.2007 Strasbourg; 10. Int Kongr DGKH, Berlin, 18.-21.4.2010. Available from: http://www.cclinparisnord.org/NCHH/2007/120607/PosterPoigneeSeguier.pdf
[10] Müller G, Kramer A. Biocompatibility index of antiseptic agents by parallel assessment of antimicrobial activity and cellular cytotoxicity. J Antimicrob Chemother. 2008;61(6):1281-7. DOI: 10.1093/jac/dkn125
[11] Kramer A, Assadian O, Christiansen B, Exner M, Gebel J, Kohnen W, Vossebein L, Zastrow KD. Gemeinsame Stellungnahme der DGKH und der Desinfektionsmittelkommission des VAH zum Stellenwert der antimikrobiellen Ausstattung von Objekten in der Infektionsprävention. Hyg Med. 2010;35(12):476-8.

