Acute abducens nerve palsy as a presenting feature in carotid-cavernous fistula in a 6-year-old girl
Neelam Pawar 1R. Ramakrishanan 1
Devendra Maheshwari 1
Meenakshi Ravindran 1
1 Aravind Eye Hospital & Postgraduate Institute of Ophthalmology, Tirunelveli, Tamil Nadu, India
Abstract
Carotid-cavernous fistulas (CCF) are abnormal communications between the internal carotid artery and the cavernous sinus. Traumatic carotid-cavernous fistulae are rare potential complications of craniofacial trauma. Typical findings of CCF are proptosis, chemosis, headache, oculomotor or abducens nerve palsy, trigeminal pain and pulsating bruit over the temporal skull and the bulb.
CCF are reported very rarely in childhood. This report describes the clinical and radiological findings of a pediatric patient presented with CCF.
Keywords
carotid-cavernous fistula, child
Case report
A 6-year-old girl in previously good health presented with acute onset of inturning of the right eye and binocular diplopia of 10 days duration. There was no associated headache and eye pain. Her mother gave history of blunt injury by umbrella over right eye 10 days back.
On examination, visual acuity without correction was 20/20 in each eye, right eye had mild conjuctival congestion and normal findings on pupillary examination. Sensorimotor examination revealed a complete abduction limitation on the right. She had an esotropia of 45 PD when examined using the modified Krimsky method. The findings were consistent with a right abducens nerve palsy. Intraocular pressures were 18 mmHg in the right eye and 17 mmHg in the left eye. Patient was advised for MRI Brain imaging but she did not report back to clinic.
She presented again after 3 weeks with features of proptosis, chemosis, engorged veins in right eye (Figure 1 [Fig. 1]). Visual acuity was 20/20 in both eyes. Slit-lamp biomicroscopy of the right eye revealed engorged episcleral vessels in a corkscrew configuration and clear cornea. Orbital and cephalic bruits were appreciated. Fundus examination revealed normal-appearing opticdisc, maculae, and retinal periphery with the exception of mild retinal vascular tortuosity in the right eye.

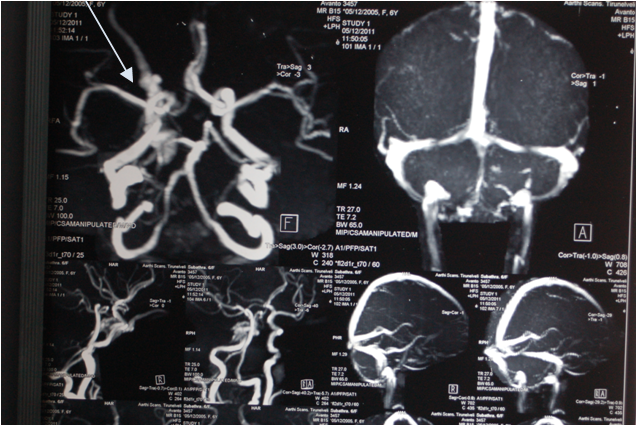
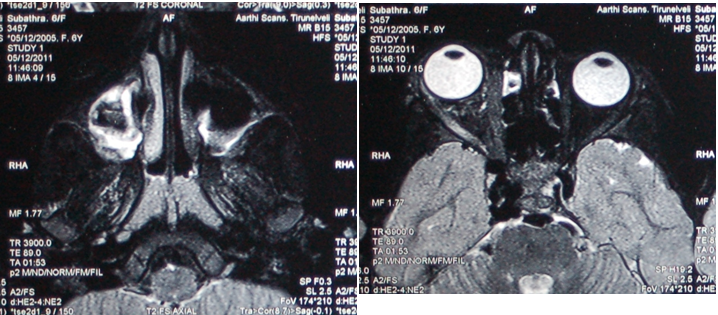
Magnetic resonance imaging (MRI) of the brain and orbits with contrast revealed fistulous communication of right cavernous sinus with enlarged right superior ophthalmic vein (SOV), enlarged right cavernous sinus with multiple flow voids, which were suggestive of carotid-cavernous fistula (Figure 2 [Fig. 2] and Figure 3 [Fig. 3]). She underwent four vessel Digital Subtraction Angiography and intervention under general anaesthesia. The angiograms showed a direct CCF on right with small communication in horizontal part of cavernous ICA. High flow shunting was seen with predominant venous drainage through dilated SOV (retrograde flow) anteriorly and petrosal sinuses posteriorly. She was diagnosed as right direct CCF TYPE A and underwent intravascular coiling by transvenous route and transarterial route with complete obliteration of fistula after consulting interventional radiologists and neurosurgeons.
Postoperatively she had no neurodeficits, proptosis and conjuctival congestion improved significantly. On follow up visit after two month she had complete resolution of esotropia, proptosis and chemosis (Figure 4 [Fig. 4]).

Discussion
Carotid-cavernous fistula (CCF) is an abnormal arteriovenous communication in the cavernous sinus. The universally adopted classification system in the CCF literature is the schema developed by Barrow and his colleagues in 1985 [1] based on angiographic studies. According to their system, there are four types of CCF [2]:
- Type A (direct): shunt between the ICA and cavernous sinus; usually associated with trauma (TCCF) and produce early signs and symptoms.
- Type B (indirect): shunt between the meningeal branches of the ICA and cavernous sinus.
- Type C (indirect): shunt between the meningeal branches of the external carotid artery and cavernous sinus.
- Type D (indirect): shunt between the meningeal branches of the ICA, external carotid artery, and cavernous sinus.
Direct CCF, classified as type A or TCCF, are high-flow shunts, which occur three times as often as the indirect types. It is this category of CCF with which surgeons managing craniofacial trauma should be most familiar. Direct CCF results from a tear in the intracavernous carotid artery. Typically, it has a high flow and usually presents with oculo-orbital venous congestive features such as pulsating exophthalmos, chemosis, orbital or cephalic bruit, impairment of vision due to hemodynamic disturbance in the optic nerve or the retina, and extra-ocular palsies with diplopia.Indirect CCF generally occurs spontaneously with subtle signs [3]. The specific diagnosis of traumatic CCF is usually not complicated, although the majority of indirect CCF are not diagnosed for weeks or even months after the onset of symptoms [2].
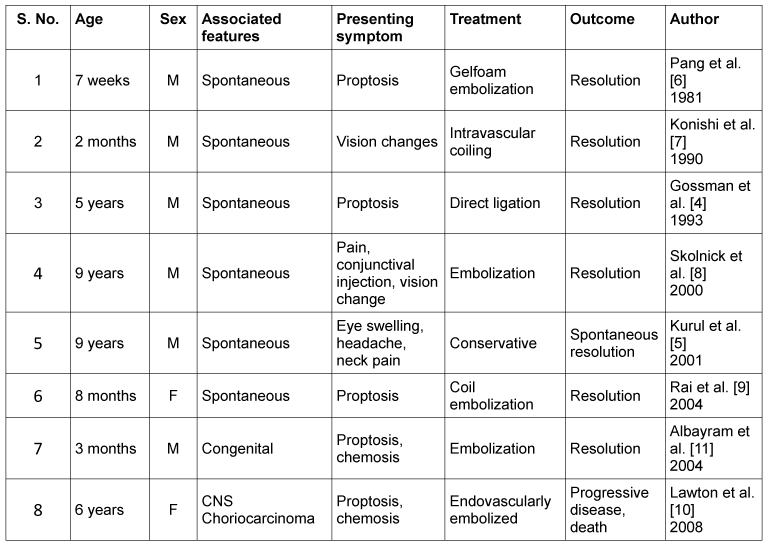
CCFs are rare in childhood and PubMed literature search reveals fewer than 10 cases in children under age 10 years (Table 1 [Tab. 1]). Spontaneous resolution has been described in children and adults [4]. We are able to find 8 reported cases in English literature using the MEDLINE search under age of 10 (Table 1 [Tab. 1]). Five of these patients required surgical intervention, such as embolization, and 1 underwent spontaneous closure [5], [6], [7], [8], [9], [10], [11]. Carotid-cavernous fistulas causing increase in intraocular pressure in infants and young children may lead to eyeball elongation and anisometropic amblyopia.
Treatment is indicated for visual compromise, or for non-resolving or progressive cavernous sinus syndrome [11]. Therapeutic embolization is indicated if there is progressive decrease in vision, ophthalmoplegia, progressive proptosis, intractable glaucoma, pain or vascular steal syndrome. Transvenous embolization via the superior ophthalmic vein or superior orbital fissure, the double-balloon embolization technique, and coil embolization modalities have been used with various success rates [2], [11].
Our patient had history of only blunt trauma with no clinical evident signs of trauma and she presented with initial acute onset of esotropia and 3 weeks later features of CCF such as proptosis, engorged vessels appeared requiring surgical intervention. She underwent intravascular coiling and complete obliteration of fistula with resolution of proptosis, chemosis,dilated episcleral vessels and esotropia.
Cases presenting with motility impairment and history of trauma should be closely observed for subtle presentation of CCF. Close observation is necessary, and surgical intervention may be indicated when there are signs of impending ocular complications.
The authors urge close observation and monitoring of visual function and early treatment of symptomatic CCF to avoid serious complications, even though spontaneous regression of CCF has been reported in some cases.
Notes
Competing interests
The authors declare that they have no competing interests.
References
[1] Barrow DL, Spector RH, Braun IF, Landman JA, Tindall SC, Tindall GT. Classification and treatment of spontaneous carotid-cavernous sinus fistulas. J Neurosurg. 1985 Feb;62(2):248-56. DOI: 10.3171/jns.1985.62.2.0248[2] Fattahi TT, Brandt MT, Jenkins WS, Steinberg B. Traumatic carotid-cavernous fistula: pathophysiology and treatment. J Craniofac Surg. 2003 Mar;14(2):240-6. DOI: 10.1097/00001665-200303000-00020
[3] Gossman MD, Berlin AJ, Weinstein MA, Hahn J, Price RL. Spontaneous direct carotid-cavernous fistula in childhood. Ophthal Plast Reconstr Surg. 1993;9(1):62-5. DOI: 10.1097/00002341-199303000-00010
[4] Kurul S, Cakmakçi H, Kovanlikaya A, Dirik E. The benign course of carotid-cavernous fistula in a child. Eur J Radiol. 2001 Aug;39(2):77-9. DOI: 10.1016/S0720-048X(01)00290-X
[5] Lau FH, Yuen HK, Rao SK, Lam DS. Spontaneous carotid cavernous fistula in a pediatric patient: case report and review of literature. J AAPOS. 2005 Jun;9(3):292-4. DOI: 10.1016/j.jaapos.2005.01.009
[6] Pang D, Kerber C, Biglan AW, Ahn HS. External carotid-cavernous fistula in infancy: case report and review of the literature. Neurosurgery. 1981 Feb;8(2):212-8. DOI: 10.1227/00006123-198102000-00011
[7] Konishi Y, Hieshima GB, Hara M, Yoshino K, Yano K, Takeuchi K. Congenital fistula of the dural carotid-cavernous sinus: case report and review of the literature. Neurosurgery. 1990 Jul;27(1):120-6. DOI: 10.1227/00006123-199007000-00018
[8] Skolnick KA, McDonnell JF. Spontaneous dural cavernous sinus fistula in a child. J AAPOS. 2000 Dec;4(6):383-5. DOI: 10.1067/mpa.2000.110341
[9] Rai AT, Sivak-Callcott JA, Larzo C, Marano GD. Direct carotid cavernous fistula in infancy: presentation and treatment. AJNR Am J Neuroradiol. 2004 Jun-Jul;25(6):1083-5.
[10] Lawton CT, Deveikis J, Rumboldt Z, Tuite G, Cavalier M. Carotid cavernous fistula in CNS choriocarcinoma. Pediatr Blood Cancer. 2008 Apr;50(4):893-5. DOI: 10.1002/pbc.21178
[11] Albayram S, Selcuk H, Ulus S, Selcuk D, Kocer N, Islak C. Endovascular treatment of a congenital dural caroticocavernous fistula. Pediatr Radiol. 2004 Aug;34(8):644-8. DOI: 10.1007/s00247-004-1163-2

